Saturday, January 28, 2006
TAC Newsletter 1/27/06
ENEWS - TREATMENT ADVOCACY CENTER
TREATMENT ADVOCACY CENTER
Visit our web site www.psychlaws.org
January 27, 2006
******************************
1. HELP MENTALLY ILL OUT OF DANGER ZONE - Albuquerque Journal, January 1, 2006
2. LOCAL LAWMAKER SAYS SHE WILL PROPOSE TREATMENT BILL IN UPCOMING LEGISLATIVE
SESSION - Las Cruces Sun News, January 15, 2006
3. DOMENICI ENDORSES N.M. LEGISLATION ON TREATING SERIOUS MENTAL ILLNESSES
BEFORE CRIMES HAPPEN - Press Release Of U.S. Senator Pete Domenici, January 14,
2006
4. HELP MENTALLY ILL GET THE TREATMENT THEY NEED - Albuquerque Journal, January
19, 2006
5. GOVERNOR BILL RICHARDSON ANNOUNCES SUPPORT FOR "KENDRA'S LAW"- Press Release
Of New Mexico Governor Bill Richardson, January 20, 2006
6. GOVERNOR SUPPORTS MANDATORY TREATMENT FOR MENTALLY ILL - Associated Press,
January 21, 2006
7. LAWYER SPEAKS ON KENDRA'S LAW; ADVOCATE SUPPORTS FORCED TREATMENT -
Albuquerque Journal, January 24, 2006
8. TRAGEDY RESULT OF STATE DENYING TRIAL, TREATMENT - Albuquerque Tribune, July
24, 2003
******************************
1. ALBUQUERQUE JOURNAL (NM), January 1, 2006
[Editor’s Note: As you will see in this edition of the E-News, the effort to
bring assisted outpatient treatment (AOT) to New Mexico has gained full steam,
experiencing one political breakthrough after another in the last weeks.
This editorial from New Mexico’s “paper of record” sets the scene as it was on
New Year’s Day, and also features two of the state’s champions for treatment.
Representative Joni Gutierrez introduced legislation that, if passed, would
bring AOT to one of the eight states without a law for it. And she did so
despite knowing that that this type of legislation could be heard in the
legislature only if one of the few bills that Governor Bill Richardson placed on
his legislative “call list.” The comments of some of the Governor’s
administrators about Rep. Gutierrez’s proposal, made a spot on that list seem a
distinctly remote possibly.
In stepped Albuquerque Mayor Martin Chávez, another hero and early proponent,
who pledged to implement AOT in his city even if the measure was not considered
in the legislature. As Mayor Chavez notes below, it would probably be the first
time that AOT has been implemented on the municipal level (a warning to
advocates who may see an opportunity – the possibility of city only adoption is
only available in Albuquerque due to some unique provisions of New Mexico law.)]
HELP MENTALLY ILL OUT OF DANGER ZONE
Editorial
In New Mexico, you have to deteriorate to the point of being dangerous before
someone can intervene and force you to get the mental-health help you need.
Albuquerque Mayor Martin Chávez and state Rep. Joni Gutierrez say help should be
available before that.
After being rebuffed by the state's Human Services and Health secretaries, the
mayor unveiled a plan Wednesday asking the City Council to pass a law allowing
mandatory outpatient treatment for people with mental illnesses.
"To my knowledge, this is the first time this is being done on a municipal
level," says Chávez, no stranger to forcing an issue he feels strongly about.
His push to register sex offenders got a reluctant state government on board
with its own program.
Human Services Secretary Pamela Hyde and Health Secretary Michelle Lujan Grisham
say the state lacks the mental health services for such a plan and they "favor
caution in this kind of government intervention in the lives of people who have
committed no crime."
If the strongest argument is lack of a place to treat the mentally ill,
Gutierrez says that perhaps some of the state's estimated $500 million in extra
revenue should be spent on the problem. And do we have to wait until a crime is
committed to help those who can't help themselves while in the throes of
schizophrenia, bipolar disorder or other serious mental illness?
New York's mandatory treatment law is credited with reducing homelessness,
hospitalization, arrests and incarcerations by 74 percent or more for patients
who have been subjected to it.
New Mexico is one of only eight states without such a law. Chilling arguments
for earlier intervene include:
2005: John Hyde, 48, is accused of killing five people, including the two police
officers trying to pick him up for a mental health evaluation. Bipolar and
schizophrenic, Hyde was off his medication, according to his family, which
desperately tried to get him help.
2003: APD Sgt. Carol Oleksak is shot in the head by Duc Minh Pham, 43, who had
schizophrenia, a brain injury and numerous run-ins with police. He, in turn, is
shot and killed by police officers.
1994: Stephen Mercer, 33, is shot and killed after shooting and killing his
father, former state Sen. Joe Mercer, and Bernalillo County Sheriff's Lt.
William Sibrava. Stephen Mercer didn't want to be taken in for a mental-health
evaluation.
Gutierrez, D-Las Cruces, took the issue up at the state level on Thursday,
announcing a bill for the upcoming legislative session that "will allow New
Mexico courts to order people who meet strict criteria for severe mental illness
into intensive and supervised outpatient treatment."
"Existing New Mexico law essentially forces people who lack insight into their
illness to hit rock bottom before they can be helped," Gutierrez says. "Forced
deterioration is cruel and inhumane."
The approach is backed by state and local chapters of the National Alliance for
Mental Illnesses. But Leslie Tremaine, the governor's adviser on behavioral
health, says the state should target resources to those who want to be treated.
"We very strongly oppose what the mayor is recommending."
Gutierrez says she understands the concern that forced treatment can infringe on
individual rights and be abused. But she says her law is crafted to prevent
that. "If there's a better solution, help us find it. We're trying to find a way
to help these families. We need something."
And at least Chávez and Gutierrez are willing to look for it before another sad
situation turns tragic.
******************************
2. LAS CRUCES SUN NEWS (NM), January 15, 2006
[Editor’s Note: In addition to the Albuquerque press conference described in
the last article, Rep. Joni Gutierrez also had one in her hometown of Las
Cruces. Although he was unfortunately unable to make his scheduled appearance,
the effort for AOT received a huge boost from her partner for the event – Pete
Domenici, one of New Mexico’s U.S. Senators and perhaps Capitol Hill’s most
influential advocate for the care of those with severe mental illness. He is
also on our Honorary Advisory Board.]
LOCAL LAWMAKER SAYS SHE WILL PROPOSE TREATMENT BILL IN UPCOMING LEGISLATIVE
SESSION
By Dolores M. Bernal, Sun-News Reporter
State Rep. Joni Gutierrez, D-Las Cruces, said Saturday she will introduce a bill
requiring New Mexico to provide treatment to those who suffer from severe mental
illnesses.
The Legislature convenes Tuesday in Santa Fe for a 30-day session.
Gutierrez said her legislation will help prevent crimes committed by people who
are mentally unstable.
"This is something new in New Mexico and is going to cause a ripple effect in
our state," said Gutierrez. "(The law) will allow treatment for a small, but
significant number of people."
Sen. Pete Domenici, R-N.M., was scheduled to attend the news conference in
support of Gutierrez's bill but was unable due to a death in the family.
"There are many mentally ill in jail and they should receive treatment,"
Domenici said over a speaker phone at the office of the National Alliance for
the Mentally Ill of Doña Ana County in downtown Las Cruces. "... They're crying
out for help."
Domenici has been a longtime advocate in Congress for the mentally ill. His
daughter suffers from schizophrenia.
The bill Gutierrez will introduce is modeled after New York's Kendra's Law --
legislation that provides for court-ordered assisted outpatient treatment or AOT
for certain people with mental illness who are unlikely to survive safely in the
community without supervision.
Some 42 other states already have AOT laws in the books, including Michigan and
Florida. New Mexico does not.
Legislators believe that having an AOT program in the state will prevent crimes
such as the one committed by Carlos Preciado Jr. of Las Cruces.
In 2005, 24-year-old Preciado struck and killed pedestrian Alvin Moore, 68, of
Las Cruces. Preciado had been diagnosed with schizophrenia, but had refused
medication.
Authorities had dealt with Preciado at least 32 times previously, according to
police.
"This death and others can be prevented and it is my belief they will with the
incorporation of this legislation," Domenici said in a letter to Gutierrez
endorsing her legislation.
Advocacy groups such as the National Alliance for the Mentally Ill said that
such legislation is overdue in New Mexico and that they will support it fully.
"We're asking anyone if they feel compelled to help us convince our fellow New
Mexicans that this is a good thing for their communities," Gutierrez said.
******************************
3. PRESS RELEASE OF U.S. SENATOR PETE DOMENICI, January 14, 2006
[Editor’s Note: Senator Domenici’s support for bringing AOT to his home state
is more than just a loan of his name. If the unusual involvement of a federal
legislator in a state legislative issue isn’t enough, this comprehensive press
release and letter from his office and for AOT makes his vigorous interest
patently clear.]
PETE V. DOMENICI
UNITED STATES SENATOR
FOR IMMEDIATE RELEASE
January 14, 2006
Contact: Chris Gallegos
DOMENICI ENDORSES N.M. LEGISLATION ON TREATING SERIOUS MENTAL ILLNESSES BEFORE
CRIMES HAPPEN
FROM THE OFFICE OF SENATOR PETE V. DOMENICI
Saturday, January 14, 2006
LAS CRUCES - U.S. Senator Pete Domenici, a long-time advocate for the mentally
ill, today endorsed proposed state legislation that would help those with
serious mental illnesses receive the care they need before their illness drives
them to commit a crime.
Domenici today joined state Representative Joni Gutierrez (D-Doña Ana) to
support her legislation to establish a judicial process allowing New Mexico
District Courts, under strict guidelines, to require intensive and supervised
outpatient treatment or assisted outpatient treatment (AOT) for some people
suffering from severe mental illnesses. New Mexico is currently one of eight
states that do not have such a policy.
Gutierrez plans to introduce the bill during the upcoming legislative session,
which begins Tuesday. Domenici presented Gutierrez with a letter of endorsement
(text included below).
“New Mexico must join the 42 other states with assisted outpatient treatment
laws. It is imperative for New Mexico to make proactive decisions to provide
clear and compassionate assistance to those who suffer from severe mental
illness,” Domenici said.
“We must have realistic solutions to stop such horrific crimes and to better
serve the mental health population. I believe Representative Gutierrez’s
proposed legislation would not only prevent possible crimes, but offer fair and
safe treatment for individuals who suffer from severe mental illnesses,” he
said.
“An AOT program will identify individuals who need the most help and support
them through an intensive and supervised outpatient treatment program. With this
legislation, I know New Mexico can positively affect many individuals who live
in the turbulent world of mental illness,” he continued.
In recent months, New Mexicans have learned the tragic consequences of severely
mentally ill persons are accused of killings related to their illnesses going
untreated. Inciting the John Hyde case in Albuquerque and the Carlos Preciado
Jr. case in Las Cruces, Domenici also pointed to the April 2000 New York Times
series, “The Well-Marked Roads to Homicidal Rage,” that analyzed the cases of
100 rampage killers across the country, 48 of which involved killers who had
some kind of formal diagnosis for a mental illness.
“Some argue that it is wrong to force individuals to undergo treatment against
their will. We argue that the tragic consequences are simply too monumental not
to require help under certain circumstances,” Domenici said. “The success rate
of the AOT program in other states has been well documented in both research and
in practice.”
Domenici cosponsored the 1999 federal law that authorized the federal mental
health court program, through which Bernalillo County has established a Mental
Health Court that operates with a separate docket and are specially geared
toward the mentally disabled, with personnel trained in understanding mental
illnesses. The court includes a training component so that law enforcement is
better able to recognize signs of mental illness.
Domenici is the author of the landmark federal 1996 Mental Health Parity law to
begin ensuring fuller insurance coverage of mental health benefits by
prohibiting a group health plan from treating mental health benefits differently
from the coverage of medical and surgical benefits. He is continuing to work on
new legislation to build on the progress made with the 1996 legislation.
-----------------
The following is the text of Domenici's letter endorsing the Gutierrez bill:
January 14, 2006
The Honorable Joni Marie Gutierrez New Mexico House of Representatives 208 North
Miranda Las Cruces, New Mexico 88005
Dear Representative Gutierrez:
I want to express my strong support for your introduction and sponsorship of new
mental health treatment legislation to create an assisted outpatient treatment
(AOT) program for individuals who suffer from severe mental illness. As you
know, I continually advocate for federal legislation regarding mental health
issues in the U.S. Senate. I believe it is imperative for New Mexico to make
proactive decisions to provide clear and compassionate assistance to those who
suffer from severe mental illness. The proposed AOT program will identify
individuals who need the most help and support them through an intensive and
supervised outpatient treatment program. With this legislation, I know New
Mexico can positively affect many individual lives who live in the turbulent
world of mental illness.
Many times we read the news and recoil in shock and disbelief at the actions
taken by individuals who were not diagnosed or who do not follow their treatment
plan. This strikes us most when we realize the results are tragedies we could
have prevented. Sadly, on August 18, 2005 the citizens of the City of
Albuquerque and the State of New Mexico learned of the tragedies that can ensue
when individuals with severe mental illness are not supported and served by the
current system. On this day, 48 year-old John Hyde allegedly shot and killed
five people. Two of whom were police officers. It has been reported by his
family that Mr. Hyde had been off his medication for schizophrenia and bipolar
disorder for at least five months. The family felt helpless to assist him and
his therapist told his family they had to wait for him to “escalate.” In the
case of Mr. Hyde, at what point do you identify an individual as escalated?
The John Hyde case is not the only incident where New Mexico law failed to help
an individual with severe mental illness. Also in 2005, 24-year-old Carlos
Preciado Jr. struck and killed 68-year-old Alvin Moore of Las Cruces. Mr.
Preciado had recently been discharged from the hospital because he was not
considered a danger to himself of others. The record shows that Mr. Preciado was
refusing medication for his diagnosed schizophrenia. Also, the record
demonstrates the police had dealt with Mr. Preciado at least 32 times in the
past. This death and others can be prevented and it is my belief they will with
the incorporation of this legislation.
Incidents such as this are not solitary and cannot be identified as “they just
snapped.” On April 10, 2000, The New York Times published a four part series of
articles titled The Well-Marked Roads to Homicidal Rage. This report analyzed
the cases of 100 rampage killers across the country. Most notably these articles
reported that of the 100 cases, 48 killers had some kind of formal diagnosis for
a mental illness. Twenty-five of the killers had received a diagnosis of mental
illness before committing their crimes. Fourteen of 24 individuals with
prescribed psychiatric drugs had stopped taking their medication prior to
committing their crimes. Also, The Times discovered that in 63 cases the killers
had previously made threats of violence, in 55 cases killers had regularly
expressed explosive anger or frustration, and in 35 cases these individuals had
a documented history of assaults and violent behavior.
As you can see, it is imperative to find realistic solutions to stop such
horrific crimes and to better serve the mental health population. I believe your
proposed legislation would not only prevent possible crimes, but offer fair and
safe treatment for individuals who suffer from severe mental illnesses.
Currently, New Mexico is one of only eight states that do not provide an AOT
service. The success rate of the AOT program in other states has been well
documented in both research and in practice. It is time for New Mexico to take
the steps to support individuals with severe mental illnesses and prevent the
possible harm to themselves and possibly others. Let us not pledge not to have
another day like August 18, 2005 in our state.
It is my hope this legislation will be accepted by both the New Mexico House of
Representatives and the Senate and signed promptly into state law. Thank you
very much for your attention to this matter, and if you need any other further
assistance in this matter please let me know
Sincerely, Pete V. Domenici United States Senator
******************************
4. ALBUQUERQUE JOURNAL, January 19, 2006
[Editor’s Note: Just as important as the legislative leaders of the campaign
for AOT in New Mexico is the tremendous grassroots effort to bring the treatment
mechanism to the state. At the head is NAMI-New Mexico. A unanimous board vote
to make AOT a priority followed up with scores of packets to legislators, office
visits both in districts and Santa Fe, and an informational lecture in the heart
of the Capitol offer only a glimpse at the breadth of its activities targeted at
bringing intensive and supervised court-ordered treatment to those most overcome
by a severe mental illness.
Particularly active has been a cadre of advocates from the Albuquerque chapter.
Below is an exceptional op-ed from NAMI-Albuquerque President Jane Lancaster.]
HELP MENTALLY ILL GET THE TREATMENT THEY NEED
By Jane Lancaster
National Alliance for Mental Illness
Assisted outpatient treatment is a court-ordered program designed to bring
intensive, consistent care to people overwhelmed by severe psychiatric
illnesses. New Mexico is one of only eight states that do not have some form of
AOT law, but that may soon change.
State Rep. Joni Gutierrez, D-Las Cruces, is advocating legislation to enable and
fund AOT. Albuquerque Mayor Martin Chávez has announced his intention to push
for an ordinance if action at the state level is delayed. U.S. Sen. Pete
Domenici endorses AOT measures as a matter of both compassion and public safety.
The proposed Albuquerque ordinance would create a psychiatric officer to
evaluate referrals and advise the Mayor's Office, which could petition District
Court to order assisted outpatient treatment, including psychiatric, medical and
social services and ensuring medications are taken as prescribed.
Before entering an order, a judge would have to find that there is no less
restrictive option for that person's care. The person with the severe mental
illness must also be unlikely to survive safely in the community and likely to
cause serious harm to self or others without the court-ordered outpatient care.
Referrals for AOT consideration can come from concerned family, physicians, the
police department's Crisis Invention Team (CIT), or the Albuquerque Family and
Community Services Department.
Based on statistics from other states, AOT might be used in Albuquerque in 35
cases a year. These AOT orders are subject to petition, limited to a period of
six months and can be extended only after review.
Albuquerque has a history of proactive mental health reform at the community
level. The city was one of the first in the country to establish a CIT, groups
of specially-trained police officers who respond to mental health calls. The CIT
follow up such calls by making connections to social and mental health workers
to ensure the individual doesn't fall through the cracks between providers.
By 2005 Albuquerque had established fully functioning mental health courts, a
jail diversion program and a Program of Assertive Community Treatment (PACT) for
individuals with mental illness and in trouble with the judicial system.
The mayor has announced that a second team is to be added to the program that
has become a national model for integrated services.
Now the community is being asked to respond again: this time, to protect the
most severely mentally ill who have no insight into their problems and who,
because of their disease, cannot cooperate on their own.
Such individuals have inconsistent care that results in repeated
hospitalizations or such nonexistent care that they require emergency services.
Reactive responses such as these deplete New Mexico's scant mental health
resources and limited hospital beds.
We can do it this year. As with the CIT and PACT teams, Albuquerque is in a
position to put the AOT program in place in 2006. At least 20 percent of
killings in Albuquerque in 2005 were associated with mental illness in which
families, bystanders, police and the mentally ill were victims.
If the state is slow to respond, let's stop these tragedies at the city level
with a proactive rather than a costly, reactive program.
Jonathan Stanley from the Treatment Advocacy Center in Arlington, Va., will
speak on assisted outpatient treatment at noon Monday at Noon Day Ministry,
Central and Broadway NE.
A lawyer who has suffered severe mental illness, Stanley has worked with many
states to develop AOT legislation modeled after Kendra's Law in New York State.
For more information about the noon event.
Jane B. Lancaster is president of the Albuquerque chapter of the National
Alliance for Mental Illness.
******************************
5. PRESS RELEASE OF NEW MEXICO GOVERNOR BILL RICHARDSON, January 20, 2006
[Editor’s Note: New Mexican advocates and political leaders fervently spoke of
the need for AOT, and Governor Bill Richardson listened. Last week he not only
announced that the AOT bill would be on his call list, he even held a press
conference to announce the decision – a strong sign that he not only thought the
measure should be debated, but that it should also be passed.]
GOVERNOR BILL RICHARDSON ANNOUNCES SUPPORT FOR "KENDRA'S LAW"
January 20, 2006
Jon Goldstein
(SANTA FE, NM) - Governor Bill Richardson today announced his support for
“Kendra’s Law,” House Bill 174, a bipartisan effort to help those with a serious
mental illness receive the care they need before their illness drives them to
commit a crime.
The Governor was joined by Representative Joni Marie Gutierrez, the bill’s
sponsor, as well as Debbie King and Susan Smith whose husbands were killed by a
behavioral health patient last August in Albuquerque, and Albuquerque Police
Sgt. Carol Oleksak who in 2003 was shot in the head by a man with both brain
injuries and schizophrenia.
“Kendra’s Law will help patients live and function in their communities by
working to get them the compassionate care and treatment they need,” said
Governor Richardson. “We need this law to prevent events like the tragic murders
in Albuquerque last summer. We have to do everything we can to prevent this from
happening to another family, another police officer, or another community, ever
again.”
Under this law, a patient’s family or doctors will be able to get a court order
to require treatment for those whose severe mental illness makes them a threat
to themselves and their community. This law, named for Kendra Webdale a New
Yorker who was pushed in front of a subway train by a schizophrenic man, is
already in place and helping people in 42 states.
“This law is all about helping those who, sadly, are too sick to help
themselves,” said Representative Joni Marie Gutierrez, sponsor of House Bill
174. “Treating this small but significant group of people will make New Mexico’s
communities safer.”
Kendra’s Law is supported by the National Alliance for Mental Illness and Jane
Lancaster, NAMI’s Albuquerque Chapter President, also joined Governor Richardson
at his afternoon press conference. Both Albuquerque Mayor Martin Chavez and U.S.
Senator Pete Domenici, have also come out in strong support of this legislation.
******************************
6. ASSOCIATED PRESS, January 21, 2006
[Editor’s Note: Governor Richardson’s press release, however, only hinted at the
true depth of his determination to secure the benefits of AOT for his state.
This comment of his did:
"This is the governor's position. ... We're for the bill. We support it
strongly, and we're going to get it passed. And that's all there is to it."]
GOVERNOR SUPPORTS MANDATORY TREATMENT FOR MENTALLY ILL
By Deborah Baker | Associated Press
Flanked by police officers' widows and an officer who survived a shooting, Gov.
Bill Richardson on Friday threw his support behind court-ordered outpatient
treatment for some mentally ill people.
It was a turnaround for the administration, which just a couple months ago had
opposed the proposal.
Under the bill, mentally ill people could be ordered by courts to get "assisted
outpatient treatment" if they were determined to be a threat to themselves or
the community. That could include medication, therapy sessions or
alcohol-and-drug counseling.
A family member, roommate, doctor, service provider, or parole or probation
officer could petition the court for the order.
Albuquerque Mayor Martin Chavez has proposed a similar ordinance for the city
and had asked Richardson to put a bill on the agenda for this session.
Two members of the governor's cabinet, Health Secretary Michelle Lujan Grisham
and Human Services Secretary Pamela Hyde, had written a letter late last year
saying they were against it -- in part because the state lacked the resources to
properly implement such a proposal.
Richardson acknowledged Friday that there had been "open dissent and
discussions" about the issue within the administration. He said after
conversations with Chavez, U.S. Sen. Pete Domenici, R-N.M., and other advocates,
he decided to back it.
"This is the governor's position. ... We're for the bill. We support it
strongly, and we're going to get it passed. And that's all there is to it,"
Richardson said at a news conference.
Grisham, who also endorsed the bill, said the administration had added $2
million to its budget for treatment programs.
Forty-two other states have a similar law, Richardson said. It's sometimes
referred to as "Kendra's Law," after Kendra Webdale, who died in New York City
in January 1999 after she was shoved in front of a subway train by a
schizophrenic who did not take his medication.
Joining administration officials at the news conference were Debbie King and
Susan Smith, whose police-officer husbands were among five people killed in
August in Albuquerque by a diagnosed schizophrenic.
Smith said lawmakers should "bridge the gap in our health-care system" by
passing the bill, which is sponsored by Rep. Joni Gutierrez, D-Las Cruces.
Sgt. Carol Oleksak, who was shot in the head on an Albuquerque street in 2003 by
a mentally ill man, said officers encounter people with mental illness every day
who need outpatient treatment.
Saying she found it "kind of surprising I'm still here," Oleksak said she has
concluded it provided her with an opportunity to "get out and get some things
changed."
The bill is also endorsed by the state chapter of the National Alliance for
Mental Illness.
******************************
7. ALBUQUERQUE JOURNAL, January 24, 2006
[Editor’s Note: The Treatment Advocacy Center has given extensive support to
the effort for AOT in New Mexico. Up until recently, that help had come via
e-mail, phone, and the postal service. This week TAC’s Jonathan Stanley and
Rosanna Esposito were able to lend a hand in person.]
LAWYER SPEAKS ON KENDRA'S LAW; ADVOCATE SUPPORTS FORCED TREATMENT
By Jackie Jadrnak, Journal Staff Reporter
Jonathan Stanley remembers being perched on a milk crate in a New York deli,
stripping off his wet clothes to thwart transmission of government agents'
deadly energy.
Now he's an attorney, a person with bipolar disorder and an advocate for early
-- and forced, if need be -- treatment for people who can't manage their mental
illnesses.
"When I was standing on that milk crate in that deli, I had no idea I was sick,"
said Stanley, assistant director of the Advocacy Treatment Center in Arlington,
Va. He spoke to a roomful of advocates in Albuquerque Monday and plans to be in
Santa Fe this morning at the Capitol to speak in favor of Kendra's Law,
introduced as House Bill 174. It allows a court to commit a mentally ill person
to outpatient treatment for the disease.
Several people raised an issue that often comes up in New Mexico: "How can this
system work if our other (mental health) system is broken?"
"This (Kendra's Law) is for the sickest of the sick," Stanley said. "This is not
a proposal to cure all the ills of your state's mental health system."
Kendra's Law would direct services to people whose illness makes them incapable
of taking care of themselves and recognizing their need for treatment, he said.
He estimated that 75 people each year in New Mexico would be court-ordered into
treatment. Under such an order, he said, mental health providers tend to
coordinate their services and do a better job of treating people.
Forty-two states have some kind of outpatient treatment law, he said. However,
he noted that many of them have the same standards for an outpatient commitment
as for an inpatient commitment: that a person be an imminent danger to himself
or others.
New Mexico's proposed law has broader standards, those that show a person is
deteriorating and could become a danger to himself or others.
Because of New Mexico's shortage of specialists, its proposed law requires a
person's mental state to be assessed by a physician, but not specifically a
psychiatrist. That drew an objection from Lorette Enochs, a local board member
for the National Alliance on Mental Illness.
"People who have a heart condition go to a heart specialist ... I'm tired of
people with mental illnesses being treated like second- class citizens," she
said, noting that drugs treating brain disorders can have serious side effects
that must be monitored by an expert.
But, in the wake of the shutdown of institutions in the 1960s, a legal means has
to be provided to get treatment to people who resist it, Stanley said.
******************************
8. ALBUQUERQUE TRIBUNE, July 24, 2003
[Editor’s Note: A year-and-a-half before the recent flurry of promising events
in New Mexico, the Treatment Advocacy Center was bringing the need for AOT to
the attention of the citizens and leaders of the state.]
TRAGEDY RESULT OF STATE DENYING TRIAL, TREATMENT
By E. Fuller Torrey, M.D., and Mary T. Zdanowicz, Esq.
Sgt. Carol Oleksak lies in a hospital bed, being treated for critical wounds
inflicted by a man who could not get access to a hospital bed to be treated for
his brain disease.
That man, Duc Minh Pham, was killed by law enforcement officers (July 7, 2003)
after critically injuring Officer Oleksak.
In the past 10 years, Pham has been charged with crimes like breaking and
entering, burglary, larceny, shoplifting and criminal damage to property - at
least 50 arrests, according to Metropolitan Court records. These charges - and
others - were regularly dismissed.
Pham had schizophrenia, which, according to news reports, rendered him
incompetent for trial. Yet New Mexico law also says that as long as he was not
dangerous, he could not be committed for treatment. Without the option for trial
and treatment, he was repeatedly released back to the streets to commit another
crime.
A better law might have saved Duc Minh Pham and Officer Carol Oleksak from their
tragic and deadly encounter - earlier intervention could also have saved New
Mexicans from the financial expense of Pham’s many arrests, incarcerations, and
court dates. Unfortunately, the revolving door of jail, hospitals, and the
streets that he was trapped in for almost a decade was halted not by a needed
change in law, but by death.
People who are rendered incompetent by severe mental illness need treatment
based on need, not on dangerousness.
And they deserve a law that supports the use of assisted outpatient treatment,
court-ordered treatment in the community. This alternative is much less
restrictive than a hospital and improves outcomes for severely mentally ill
individuals.
People with severe mental illnesses are about four times more likely to be
killed in an encounter with law enforcement than the general public; and the
risk to law enforcement officers, as became sadly apparent in this case, is
extremely high.
Even if a deadly encounter is averted, correctional officials often become the
caretakers of people lost to these treatable illnesses.
Nationally, 16% of incarcerated people have a severe mental illness. In New
Mexico, people with severe mental illnesses are incarcerated than are housed in
the state’s remaining psychiatric hospitals. Pham himself was jailed repeatedly,
sometimes for a few days, sometimes for months at a time.
By contrast, those placed under New York’s assisted outpatient treatment law had
an 86% reduction in incarcerations.
Kendra’s Law participants also experienced an 86% reduction in homelessness.
Approximately one-third of the homeless population have a severe mental illness
- at times including Pham, whose existence on the streets is what led to his
first encounter with police.
The New York program saw an 83% reduction in arrests. This could have helped
Pham, arrested more than 50 times and arrested for everything from disorderly
conduct to assaulting a police officer.
All New Mexicans could benefit from significant reductions in harmful behaviors,
such as harm to self (45% reduction in New York) and harm to others (44%
reduction).
New Mexico’s law ignores that the majority of those not receiving treatment for
severe mental illnesses do not believe - indeed, are rendered physiologically
incapable of understanding - that they are sick. Most will only accept treatment
if ordered to do so.
In such circumstances, the battle to be returned to competency is the true civil
rights issue, not the false “right” to be and remain psychotic.
And New Mexico law ignores that early intervention is important for clinical
reasons, as well as for public safety. Studies have shown that delayed treatment
increases treatment resistance, worsens severity of symptoms, increases
hospitalizations, and delays remission of symptoms.
Waiting to intervene can condemn someone to a lifetime of more severe and
continual illness.
New York’s law is named after Kendra Webdale, the victim of a man with untreated
schizophrenia. Perhaps New Mexico should consider Carol’s Law - for a law
enforcement officer who fell victim to the law she had sworn to uphold.
E. Fuller Torrey, M.D., is president and Mary T. Zdanowicz is executive director
of the Treatment Advocacy Center in Arlington, Va., www.psychlaws.org, a
national nonprofit organization working to eliminate barriers to treatment of
severe mental illness.
******************************
Treatment Advocacy Center E-NEWS is a publication of the Treatment Advocacy
Center.
This E-NEWS is provided as a public service by the Treatment Advocacy Center.
There is no fee. If you would also like to receive a free subscription to the
Catalyst, our quarterly hardcopy newsletter, please forward your mailing address
to info@psychlaws.org.
The Center does not accept donations from pharmaceutical companies. Support
from individuals who share our mission, however, is essential to our ability to
effectively help our most vulnerable citizens. The Treatment Advocacy Center is
a 501(c)(3) not-for-profit organization. All contributions are tax-deductible
to the extent allowed by law. Donations to the Treatment Advocacy Center should
be sent to:
Treatment Advocacy Center
200 North Glebe Road, Suite 730
Arlington, VA 22203
703-294-6001 (main no.)
703-294-6010 (fax)
TREATMENT ADVOCACY CENTER
Visit our web site www.psychlaws.org
January 27, 2006
******************************
1. HELP MENTALLY ILL OUT OF DANGER ZONE - Albuquerque Journal, January 1, 2006
2. LOCAL LAWMAKER SAYS SHE WILL PROPOSE TREATMENT BILL IN UPCOMING LEGISLATIVE
SESSION - Las Cruces Sun News, January 15, 2006
3. DOMENICI ENDORSES N.M. LEGISLATION ON TREATING SERIOUS MENTAL ILLNESSES
BEFORE CRIMES HAPPEN - Press Release Of U.S. Senator Pete Domenici, January 14,
2006
4. HELP MENTALLY ILL GET THE TREATMENT THEY NEED - Albuquerque Journal, January
19, 2006
5. GOVERNOR BILL RICHARDSON ANNOUNCES SUPPORT FOR "KENDRA'S LAW"- Press Release
Of New Mexico Governor Bill Richardson, January 20, 2006
6. GOVERNOR SUPPORTS MANDATORY TREATMENT FOR MENTALLY ILL - Associated Press,
January 21, 2006
7. LAWYER SPEAKS ON KENDRA'S LAW; ADVOCATE SUPPORTS FORCED TREATMENT -
Albuquerque Journal, January 24, 2006
8. TRAGEDY RESULT OF STATE DENYING TRIAL, TREATMENT - Albuquerque Tribune, July
24, 2003
******************************
1. ALBUQUERQUE JOURNAL (NM), January 1, 2006
[Editor’s Note: As you will see in this edition of the E-News, the effort to
bring assisted outpatient treatment (AOT) to New Mexico has gained full steam,
experiencing one political breakthrough after another in the last weeks.
This editorial from New Mexico’s “paper of record” sets the scene as it was on
New Year’s Day, and also features two of the state’s champions for treatment.
Representative Joni Gutierrez introduced legislation that, if passed, would
bring AOT to one of the eight states without a law for it. And she did so
despite knowing that that this type of legislation could be heard in the
legislature only if one of the few bills that Governor Bill Richardson placed on
his legislative “call list.” The comments of some of the Governor’s
administrators about Rep. Gutierrez’s proposal, made a spot on that list seem a
distinctly remote possibly.
In stepped Albuquerque Mayor Martin Chávez, another hero and early proponent,
who pledged to implement AOT in his city even if the measure was not considered
in the legislature. As Mayor Chavez notes below, it would probably be the first
time that AOT has been implemented on the municipal level (a warning to
advocates who may see an opportunity – the possibility of city only adoption is
only available in Albuquerque due to some unique provisions of New Mexico law.)]
HELP MENTALLY ILL OUT OF DANGER ZONE
Editorial
In New Mexico, you have to deteriorate to the point of being dangerous before
someone can intervene and force you to get the mental-health help you need.
Albuquerque Mayor Martin Chávez and state Rep. Joni Gutierrez say help should be
available before that.
After being rebuffed by the state's Human Services and Health secretaries, the
mayor unveiled a plan Wednesday asking the City Council to pass a law allowing
mandatory outpatient treatment for people with mental illnesses.
"To my knowledge, this is the first time this is being done on a municipal
level," says Chávez, no stranger to forcing an issue he feels strongly about.
His push to register sex offenders got a reluctant state government on board
with its own program.
Human Services Secretary Pamela Hyde and Health Secretary Michelle Lujan Grisham
say the state lacks the mental health services for such a plan and they "favor
caution in this kind of government intervention in the lives of people who have
committed no crime."
If the strongest argument is lack of a place to treat the mentally ill,
Gutierrez says that perhaps some of the state's estimated $500 million in extra
revenue should be spent on the problem. And do we have to wait until a crime is
committed to help those who can't help themselves while in the throes of
schizophrenia, bipolar disorder or other serious mental illness?
New York's mandatory treatment law is credited with reducing homelessness,
hospitalization, arrests and incarcerations by 74 percent or more for patients
who have been subjected to it.
New Mexico is one of only eight states without such a law. Chilling arguments
for earlier intervene include:
2005: John Hyde, 48, is accused of killing five people, including the two police
officers trying to pick him up for a mental health evaluation. Bipolar and
schizophrenic, Hyde was off his medication, according to his family, which
desperately tried to get him help.
2003: APD Sgt. Carol Oleksak is shot in the head by Duc Minh Pham, 43, who had
schizophrenia, a brain injury and numerous run-ins with police. He, in turn, is
shot and killed by police officers.
1994: Stephen Mercer, 33, is shot and killed after shooting and killing his
father, former state Sen. Joe Mercer, and Bernalillo County Sheriff's Lt.
William Sibrava. Stephen Mercer didn't want to be taken in for a mental-health
evaluation.
Gutierrez, D-Las Cruces, took the issue up at the state level on Thursday,
announcing a bill for the upcoming legislative session that "will allow New
Mexico courts to order people who meet strict criteria for severe mental illness
into intensive and supervised outpatient treatment."
"Existing New Mexico law essentially forces people who lack insight into their
illness to hit rock bottom before they can be helped," Gutierrez says. "Forced
deterioration is cruel and inhumane."
The approach is backed by state and local chapters of the National Alliance for
Mental Illnesses. But Leslie Tremaine, the governor's adviser on behavioral
health, says the state should target resources to those who want to be treated.
"We very strongly oppose what the mayor is recommending."
Gutierrez says she understands the concern that forced treatment can infringe on
individual rights and be abused. But she says her law is crafted to prevent
that. "If there's a better solution, help us find it. We're trying to find a way
to help these families. We need something."
And at least Chávez and Gutierrez are willing to look for it before another sad
situation turns tragic.
******************************
2. LAS CRUCES SUN NEWS (NM), January 15, 2006
[Editor’s Note: In addition to the Albuquerque press conference described in
the last article, Rep. Joni Gutierrez also had one in her hometown of Las
Cruces. Although he was unfortunately unable to make his scheduled appearance,
the effort for AOT received a huge boost from her partner for the event – Pete
Domenici, one of New Mexico’s U.S. Senators and perhaps Capitol Hill’s most
influential advocate for the care of those with severe mental illness. He is
also on our Honorary Advisory Board.]
LOCAL LAWMAKER SAYS SHE WILL PROPOSE TREATMENT BILL IN UPCOMING LEGISLATIVE
SESSION
By Dolores M. Bernal, Sun-News Reporter
State Rep. Joni Gutierrez, D-Las Cruces, said Saturday she will introduce a bill
requiring New Mexico to provide treatment to those who suffer from severe mental
illnesses.
The Legislature convenes Tuesday in Santa Fe for a 30-day session.
Gutierrez said her legislation will help prevent crimes committed by people who
are mentally unstable.
"This is something new in New Mexico and is going to cause a ripple effect in
our state," said Gutierrez. "(The law) will allow treatment for a small, but
significant number of people."
Sen. Pete Domenici, R-N.M., was scheduled to attend the news conference in
support of Gutierrez's bill but was unable due to a death in the family.
"There are many mentally ill in jail and they should receive treatment,"
Domenici said over a speaker phone at the office of the National Alliance for
the Mentally Ill of Doña Ana County in downtown Las Cruces. "... They're crying
out for help."
Domenici has been a longtime advocate in Congress for the mentally ill. His
daughter suffers from schizophrenia.
The bill Gutierrez will introduce is modeled after New York's Kendra's Law --
legislation that provides for court-ordered assisted outpatient treatment or AOT
for certain people with mental illness who are unlikely to survive safely in the
community without supervision.
Some 42 other states already have AOT laws in the books, including Michigan and
Florida. New Mexico does not.
Legislators believe that having an AOT program in the state will prevent crimes
such as the one committed by Carlos Preciado Jr. of Las Cruces.
In 2005, 24-year-old Preciado struck and killed pedestrian Alvin Moore, 68, of
Las Cruces. Preciado had been diagnosed with schizophrenia, but had refused
medication.
Authorities had dealt with Preciado at least 32 times previously, according to
police.
"This death and others can be prevented and it is my belief they will with the
incorporation of this legislation," Domenici said in a letter to Gutierrez
endorsing her legislation.
Advocacy groups such as the National Alliance for the Mentally Ill said that
such legislation is overdue in New Mexico and that they will support it fully.
"We're asking anyone if they feel compelled to help us convince our fellow New
Mexicans that this is a good thing for their communities," Gutierrez said.
******************************
3. PRESS RELEASE OF U.S. SENATOR PETE DOMENICI, January 14, 2006
[Editor’s Note: Senator Domenici’s support for bringing AOT to his home state
is more than just a loan of his name. If the unusual involvement of a federal
legislator in a state legislative issue isn’t enough, this comprehensive press
release and letter from his office and for AOT makes his vigorous interest
patently clear.]
PETE V. DOMENICI
UNITED STATES SENATOR
FOR IMMEDIATE RELEASE
January 14, 2006
Contact: Chris Gallegos
DOMENICI ENDORSES N.M. LEGISLATION ON TREATING SERIOUS MENTAL ILLNESSES BEFORE
CRIMES HAPPEN
FROM THE OFFICE OF SENATOR PETE V. DOMENICI
Saturday, January 14, 2006
LAS CRUCES - U.S. Senator Pete Domenici, a long-time advocate for the mentally
ill, today endorsed proposed state legislation that would help those with
serious mental illnesses receive the care they need before their illness drives
them to commit a crime.
Domenici today joined state Representative Joni Gutierrez (D-Doña Ana) to
support her legislation to establish a judicial process allowing New Mexico
District Courts, under strict guidelines, to require intensive and supervised
outpatient treatment or assisted outpatient treatment (AOT) for some people
suffering from severe mental illnesses. New Mexico is currently one of eight
states that do not have such a policy.
Gutierrez plans to introduce the bill during the upcoming legislative session,
which begins Tuesday. Domenici presented Gutierrez with a letter of endorsement
(text included below).
“New Mexico must join the 42 other states with assisted outpatient treatment
laws. It is imperative for New Mexico to make proactive decisions to provide
clear and compassionate assistance to those who suffer from severe mental
illness,” Domenici said.
“We must have realistic solutions to stop such horrific crimes and to better
serve the mental health population. I believe Representative Gutierrez’s
proposed legislation would not only prevent possible crimes, but offer fair and
safe treatment for individuals who suffer from severe mental illnesses,” he
said.
“An AOT program will identify individuals who need the most help and support
them through an intensive and supervised outpatient treatment program. With this
legislation, I know New Mexico can positively affect many individuals who live
in the turbulent world of mental illness,” he continued.
In recent months, New Mexicans have learned the tragic consequences of severely
mentally ill persons are accused of killings related to their illnesses going
untreated. Inciting the John Hyde case in Albuquerque and the Carlos Preciado
Jr. case in Las Cruces, Domenici also pointed to the April 2000 New York Times
series, “The Well-Marked Roads to Homicidal Rage,” that analyzed the cases of
100 rampage killers across the country, 48 of which involved killers who had
some kind of formal diagnosis for a mental illness.
“Some argue that it is wrong to force individuals to undergo treatment against
their will. We argue that the tragic consequences are simply too monumental not
to require help under certain circumstances,” Domenici said. “The success rate
of the AOT program in other states has been well documented in both research and
in practice.”
Domenici cosponsored the 1999 federal law that authorized the federal mental
health court program, through which Bernalillo County has established a Mental
Health Court that operates with a separate docket and are specially geared
toward the mentally disabled, with personnel trained in understanding mental
illnesses. The court includes a training component so that law enforcement is
better able to recognize signs of mental illness.
Domenici is the author of the landmark federal 1996 Mental Health Parity law to
begin ensuring fuller insurance coverage of mental health benefits by
prohibiting a group health plan from treating mental health benefits differently
from the coverage of medical and surgical benefits. He is continuing to work on
new legislation to build on the progress made with the 1996 legislation.
-----------------
The following is the text of Domenici's letter endorsing the Gutierrez bill:
January 14, 2006
The Honorable Joni Marie Gutierrez New Mexico House of Representatives 208 North
Miranda Las Cruces, New Mexico 88005
Dear Representative Gutierrez:
I want to express my strong support for your introduction and sponsorship of new
mental health treatment legislation to create an assisted outpatient treatment
(AOT) program for individuals who suffer from severe mental illness. As you
know, I continually advocate for federal legislation regarding mental health
issues in the U.S. Senate. I believe it is imperative for New Mexico to make
proactive decisions to provide clear and compassionate assistance to those who
suffer from severe mental illness. The proposed AOT program will identify
individuals who need the most help and support them through an intensive and
supervised outpatient treatment program. With this legislation, I know New
Mexico can positively affect many individual lives who live in the turbulent
world of mental illness.
Many times we read the news and recoil in shock and disbelief at the actions
taken by individuals who were not diagnosed or who do not follow their treatment
plan. This strikes us most when we realize the results are tragedies we could
have prevented. Sadly, on August 18, 2005 the citizens of the City of
Albuquerque and the State of New Mexico learned of the tragedies that can ensue
when individuals with severe mental illness are not supported and served by the
current system. On this day, 48 year-old John Hyde allegedly shot and killed
five people. Two of whom were police officers. It has been reported by his
family that Mr. Hyde had been off his medication for schizophrenia and bipolar
disorder for at least five months. The family felt helpless to assist him and
his therapist told his family they had to wait for him to “escalate.” In the
case of Mr. Hyde, at what point do you identify an individual as escalated?
The John Hyde case is not the only incident where New Mexico law failed to help
an individual with severe mental illness. Also in 2005, 24-year-old Carlos
Preciado Jr. struck and killed 68-year-old Alvin Moore of Las Cruces. Mr.
Preciado had recently been discharged from the hospital because he was not
considered a danger to himself of others. The record shows that Mr. Preciado was
refusing medication for his diagnosed schizophrenia. Also, the record
demonstrates the police had dealt with Mr. Preciado at least 32 times in the
past. This death and others can be prevented and it is my belief they will with
the incorporation of this legislation.
Incidents such as this are not solitary and cannot be identified as “they just
snapped.” On April 10, 2000, The New York Times published a four part series of
articles titled The Well-Marked Roads to Homicidal Rage. This report analyzed
the cases of 100 rampage killers across the country. Most notably these articles
reported that of the 100 cases, 48 killers had some kind of formal diagnosis for
a mental illness. Twenty-five of the killers had received a diagnosis of mental
illness before committing their crimes. Fourteen of 24 individuals with
prescribed psychiatric drugs had stopped taking their medication prior to
committing their crimes. Also, The Times discovered that in 63 cases the killers
had previously made threats of violence, in 55 cases killers had regularly
expressed explosive anger or frustration, and in 35 cases these individuals had
a documented history of assaults and violent behavior.
As you can see, it is imperative to find realistic solutions to stop such
horrific crimes and to better serve the mental health population. I believe your
proposed legislation would not only prevent possible crimes, but offer fair and
safe treatment for individuals who suffer from severe mental illnesses.
Currently, New Mexico is one of only eight states that do not provide an AOT
service. The success rate of the AOT program in other states has been well
documented in both research and in practice. It is time for New Mexico to take
the steps to support individuals with severe mental illnesses and prevent the
possible harm to themselves and possibly others. Let us not pledge not to have
another day like August 18, 2005 in our state.
It is my hope this legislation will be accepted by both the New Mexico House of
Representatives and the Senate and signed promptly into state law. Thank you
very much for your attention to this matter, and if you need any other further
assistance in this matter please let me know
Sincerely, Pete V. Domenici United States Senator
******************************
4. ALBUQUERQUE JOURNAL, January 19, 2006
[Editor’s Note: Just as important as the legislative leaders of the campaign
for AOT in New Mexico is the tremendous grassroots effort to bring the treatment
mechanism to the state. At the head is NAMI-New Mexico. A unanimous board vote
to make AOT a priority followed up with scores of packets to legislators, office
visits both in districts and Santa Fe, and an informational lecture in the heart
of the Capitol offer only a glimpse at the breadth of its activities targeted at
bringing intensive and supervised court-ordered treatment to those most overcome
by a severe mental illness.
Particularly active has been a cadre of advocates from the Albuquerque chapter.
Below is an exceptional op-ed from NAMI-Albuquerque President Jane Lancaster.]
HELP MENTALLY ILL GET THE TREATMENT THEY NEED
By Jane Lancaster
National Alliance for Mental Illness
Assisted outpatient treatment is a court-ordered program designed to bring
intensive, consistent care to people overwhelmed by severe psychiatric
illnesses. New Mexico is one of only eight states that do not have some form of
AOT law, but that may soon change.
State Rep. Joni Gutierrez, D-Las Cruces, is advocating legislation to enable and
fund AOT. Albuquerque Mayor Martin Chávez has announced his intention to push
for an ordinance if action at the state level is delayed. U.S. Sen. Pete
Domenici endorses AOT measures as a matter of both compassion and public safety.
The proposed Albuquerque ordinance would create a psychiatric officer to
evaluate referrals and advise the Mayor's Office, which could petition District
Court to order assisted outpatient treatment, including psychiatric, medical and
social services and ensuring medications are taken as prescribed.
Before entering an order, a judge would have to find that there is no less
restrictive option for that person's care. The person with the severe mental
illness must also be unlikely to survive safely in the community and likely to
cause serious harm to self or others without the court-ordered outpatient care.
Referrals for AOT consideration can come from concerned family, physicians, the
police department's Crisis Invention Team (CIT), or the Albuquerque Family and
Community Services Department.
Based on statistics from other states, AOT might be used in Albuquerque in 35
cases a year. These AOT orders are subject to petition, limited to a period of
six months and can be extended only after review.
Albuquerque has a history of proactive mental health reform at the community
level. The city was one of the first in the country to establish a CIT, groups
of specially-trained police officers who respond to mental health calls. The CIT
follow up such calls by making connections to social and mental health workers
to ensure the individual doesn't fall through the cracks between providers.
By 2005 Albuquerque had established fully functioning mental health courts, a
jail diversion program and a Program of Assertive Community Treatment (PACT) for
individuals with mental illness and in trouble with the judicial system.
The mayor has announced that a second team is to be added to the program that
has become a national model for integrated services.
Now the community is being asked to respond again: this time, to protect the
most severely mentally ill who have no insight into their problems and who,
because of their disease, cannot cooperate on their own.
Such individuals have inconsistent care that results in repeated
hospitalizations or such nonexistent care that they require emergency services.
Reactive responses such as these deplete New Mexico's scant mental health
resources and limited hospital beds.
We can do it this year. As with the CIT and PACT teams, Albuquerque is in a
position to put the AOT program in place in 2006. At least 20 percent of
killings in Albuquerque in 2005 were associated with mental illness in which
families, bystanders, police and the mentally ill were victims.
If the state is slow to respond, let's stop these tragedies at the city level
with a proactive rather than a costly, reactive program.
Jonathan Stanley from the Treatment Advocacy Center in Arlington, Va., will
speak on assisted outpatient treatment at noon Monday at Noon Day Ministry,
Central and Broadway NE.
A lawyer who has suffered severe mental illness, Stanley has worked with many
states to develop AOT legislation modeled after Kendra's Law in New York State.
For more information about the noon event.
Jane B. Lancaster is president of the Albuquerque chapter of the National
Alliance for Mental Illness.
******************************
5. PRESS RELEASE OF NEW MEXICO GOVERNOR BILL RICHARDSON, January 20, 2006
[Editor’s Note: New Mexican advocates and political leaders fervently spoke of
the need for AOT, and Governor Bill Richardson listened. Last week he not only
announced that the AOT bill would be on his call list, he even held a press
conference to announce the decision – a strong sign that he not only thought the
measure should be debated, but that it should also be passed.]
GOVERNOR BILL RICHARDSON ANNOUNCES SUPPORT FOR "KENDRA'S LAW"
January 20, 2006
Jon Goldstein
(SANTA FE, NM) - Governor Bill Richardson today announced his support for
“Kendra’s Law,” House Bill 174, a bipartisan effort to help those with a serious
mental illness receive the care they need before their illness drives them to
commit a crime.
The Governor was joined by Representative Joni Marie Gutierrez, the bill’s
sponsor, as well as Debbie King and Susan Smith whose husbands were killed by a
behavioral health patient last August in Albuquerque, and Albuquerque Police
Sgt. Carol Oleksak who in 2003 was shot in the head by a man with both brain
injuries and schizophrenia.
“Kendra’s Law will help patients live and function in their communities by
working to get them the compassionate care and treatment they need,” said
Governor Richardson. “We need this law to prevent events like the tragic murders
in Albuquerque last summer. We have to do everything we can to prevent this from
happening to another family, another police officer, or another community, ever
again.”
Under this law, a patient’s family or doctors will be able to get a court order
to require treatment for those whose severe mental illness makes them a threat
to themselves and their community. This law, named for Kendra Webdale a New
Yorker who was pushed in front of a subway train by a schizophrenic man, is
already in place and helping people in 42 states.
“This law is all about helping those who, sadly, are too sick to help
themselves,” said Representative Joni Marie Gutierrez, sponsor of House Bill
174. “Treating this small but significant group of people will make New Mexico’s
communities safer.”
Kendra’s Law is supported by the National Alliance for Mental Illness and Jane
Lancaster, NAMI’s Albuquerque Chapter President, also joined Governor Richardson
at his afternoon press conference. Both Albuquerque Mayor Martin Chavez and U.S.
Senator Pete Domenici, have also come out in strong support of this legislation.
******************************
6. ASSOCIATED PRESS, January 21, 2006
[Editor’s Note: Governor Richardson’s press release, however, only hinted at the
true depth of his determination to secure the benefits of AOT for his state.
This comment of his did:
"This is the governor's position. ... We're for the bill. We support it
strongly, and we're going to get it passed. And that's all there is to it."]
GOVERNOR SUPPORTS MANDATORY TREATMENT FOR MENTALLY ILL
By Deborah Baker | Associated Press
Flanked by police officers' widows and an officer who survived a shooting, Gov.
Bill Richardson on Friday threw his support behind court-ordered outpatient
treatment for some mentally ill people.
It was a turnaround for the administration, which just a couple months ago had
opposed the proposal.
Under the bill, mentally ill people could be ordered by courts to get "assisted
outpatient treatment" if they were determined to be a threat to themselves or
the community. That could include medication, therapy sessions or
alcohol-and-drug counseling.
A family member, roommate, doctor, service provider, or parole or probation
officer could petition the court for the order.
Albuquerque Mayor Martin Chavez has proposed a similar ordinance for the city
and had asked Richardson to put a bill on the agenda for this session.
Two members of the governor's cabinet, Health Secretary Michelle Lujan Grisham
and Human Services Secretary Pamela Hyde, had written a letter late last year
saying they were against it -- in part because the state lacked the resources to
properly implement such a proposal.
Richardson acknowledged Friday that there had been "open dissent and
discussions" about the issue within the administration. He said after
conversations with Chavez, U.S. Sen. Pete Domenici, R-N.M., and other advocates,
he decided to back it.
"This is the governor's position. ... We're for the bill. We support it
strongly, and we're going to get it passed. And that's all there is to it,"
Richardson said at a news conference.
Grisham, who also endorsed the bill, said the administration had added $2
million to its budget for treatment programs.
Forty-two other states have a similar law, Richardson said. It's sometimes
referred to as "Kendra's Law," after Kendra Webdale, who died in New York City
in January 1999 after she was shoved in front of a subway train by a
schizophrenic who did not take his medication.
Joining administration officials at the news conference were Debbie King and
Susan Smith, whose police-officer husbands were among five people killed in
August in Albuquerque by a diagnosed schizophrenic.
Smith said lawmakers should "bridge the gap in our health-care system" by
passing the bill, which is sponsored by Rep. Joni Gutierrez, D-Las Cruces.
Sgt. Carol Oleksak, who was shot in the head on an Albuquerque street in 2003 by
a mentally ill man, said officers encounter people with mental illness every day
who need outpatient treatment.
Saying she found it "kind of surprising I'm still here," Oleksak said she has
concluded it provided her with an opportunity to "get out and get some things
changed."
The bill is also endorsed by the state chapter of the National Alliance for
Mental Illness.
******************************
7. ALBUQUERQUE JOURNAL, January 24, 2006
[Editor’s Note: The Treatment Advocacy Center has given extensive support to
the effort for AOT in New Mexico. Up until recently, that help had come via
e-mail, phone, and the postal service. This week TAC’s Jonathan Stanley and
Rosanna Esposito were able to lend a hand in person.]
LAWYER SPEAKS ON KENDRA'S LAW; ADVOCATE SUPPORTS FORCED TREATMENT
By Jackie Jadrnak, Journal Staff Reporter
Jonathan Stanley remembers being perched on a milk crate in a New York deli,
stripping off his wet clothes to thwart transmission of government agents'
deadly energy.
Now he's an attorney, a person with bipolar disorder and an advocate for early
-- and forced, if need be -- treatment for people who can't manage their mental
illnesses.
"When I was standing on that milk crate in that deli, I had no idea I was sick,"
said Stanley, assistant director of the Advocacy Treatment Center in Arlington,
Va. He spoke to a roomful of advocates in Albuquerque Monday and plans to be in
Santa Fe this morning at the Capitol to speak in favor of Kendra's Law,
introduced as House Bill 174. It allows a court to commit a mentally ill person
to outpatient treatment for the disease.
Several people raised an issue that often comes up in New Mexico: "How can this
system work if our other (mental health) system is broken?"
"This (Kendra's Law) is for the sickest of the sick," Stanley said. "This is not
a proposal to cure all the ills of your state's mental health system."
Kendra's Law would direct services to people whose illness makes them incapable
of taking care of themselves and recognizing their need for treatment, he said.
He estimated that 75 people each year in New Mexico would be court-ordered into
treatment. Under such an order, he said, mental health providers tend to
coordinate their services and do a better job of treating people.
Forty-two states have some kind of outpatient treatment law, he said. However,
he noted that many of them have the same standards for an outpatient commitment
as for an inpatient commitment: that a person be an imminent danger to himself
or others.
New Mexico's proposed law has broader standards, those that show a person is
deteriorating and could become a danger to himself or others.
Because of New Mexico's shortage of specialists, its proposed law requires a
person's mental state to be assessed by a physician, but not specifically a
psychiatrist. That drew an objection from Lorette Enochs, a local board member
for the National Alliance on Mental Illness.
"People who have a heart condition go to a heart specialist ... I'm tired of
people with mental illnesses being treated like second- class citizens," she
said, noting that drugs treating brain disorders can have serious side effects
that must be monitored by an expert.
But, in the wake of the shutdown of institutions in the 1960s, a legal means has
to be provided to get treatment to people who resist it, Stanley said.
******************************
8. ALBUQUERQUE TRIBUNE, July 24, 2003
[Editor’s Note: A year-and-a-half before the recent flurry of promising events
in New Mexico, the Treatment Advocacy Center was bringing the need for AOT to
the attention of the citizens and leaders of the state.]
TRAGEDY RESULT OF STATE DENYING TRIAL, TREATMENT
By E. Fuller Torrey, M.D., and Mary T. Zdanowicz, Esq.
Sgt. Carol Oleksak lies in a hospital bed, being treated for critical wounds
inflicted by a man who could not get access to a hospital bed to be treated for
his brain disease.
That man, Duc Minh Pham, was killed by law enforcement officers (July 7, 2003)
after critically injuring Officer Oleksak.
In the past 10 years, Pham has been charged with crimes like breaking and
entering, burglary, larceny, shoplifting and criminal damage to property - at
least 50 arrests, according to Metropolitan Court records. These charges - and
others - were regularly dismissed.
Pham had schizophrenia, which, according to news reports, rendered him
incompetent for trial. Yet New Mexico law also says that as long as he was not
dangerous, he could not be committed for treatment. Without the option for trial
and treatment, he was repeatedly released back to the streets to commit another
crime.
A better law might have saved Duc Minh Pham and Officer Carol Oleksak from their
tragic and deadly encounter - earlier intervention could also have saved New
Mexicans from the financial expense of Pham’s many arrests, incarcerations, and
court dates. Unfortunately, the revolving door of jail, hospitals, and the
streets that he was trapped in for almost a decade was halted not by a needed
change in law, but by death.
People who are rendered incompetent by severe mental illness need treatment
based on need, not on dangerousness.
And they deserve a law that supports the use of assisted outpatient treatment,
court-ordered treatment in the community. This alternative is much less
restrictive than a hospital and improves outcomes for severely mentally ill
individuals.
People with severe mental illnesses are about four times more likely to be
killed in an encounter with law enforcement than the general public; and the
risk to law enforcement officers, as became sadly apparent in this case, is
extremely high.
Even if a deadly encounter is averted, correctional officials often become the
caretakers of people lost to these treatable illnesses.
Nationally, 16% of incarcerated people have a severe mental illness. In New
Mexico, people with severe mental illnesses are incarcerated than are housed in
the state’s remaining psychiatric hospitals. Pham himself was jailed repeatedly,
sometimes for a few days, sometimes for months at a time.
By contrast, those placed under New York’s assisted outpatient treatment law had
an 86% reduction in incarcerations.
Kendra’s Law participants also experienced an 86% reduction in homelessness.
Approximately one-third of the homeless population have a severe mental illness
- at times including Pham, whose existence on the streets is what led to his
first encounter with police.
The New York program saw an 83% reduction in arrests. This could have helped
Pham, arrested more than 50 times and arrested for everything from disorderly
conduct to assaulting a police officer.
All New Mexicans could benefit from significant reductions in harmful behaviors,
such as harm to self (45% reduction in New York) and harm to others (44%
reduction).
New Mexico’s law ignores that the majority of those not receiving treatment for
severe mental illnesses do not believe - indeed, are rendered physiologically
incapable of understanding - that they are sick. Most will only accept treatment
if ordered to do so.
In such circumstances, the battle to be returned to competency is the true civil
rights issue, not the false “right” to be and remain psychotic.
And New Mexico law ignores that early intervention is important for clinical
reasons, as well as for public safety. Studies have shown that delayed treatment
increases treatment resistance, worsens severity of symptoms, increases
hospitalizations, and delays remission of symptoms.
Waiting to intervene can condemn someone to a lifetime of more severe and
continual illness.
New York’s law is named after Kendra Webdale, the victim of a man with untreated
schizophrenia. Perhaps New Mexico should consider Carol’s Law - for a law
enforcement officer who fell victim to the law she had sworn to uphold.
E. Fuller Torrey, M.D., is president and Mary T. Zdanowicz is executive director
of the Treatment Advocacy Center in Arlington, Va., www.psychlaws.org, a
national nonprofit organization working to eliminate barriers to treatment of
severe mental illness.
******************************
Treatment Advocacy Center E-NEWS is a publication of the Treatment Advocacy
Center.
This E-NEWS is provided as a public service by the Treatment Advocacy Center.
There is no fee. If you would also like to receive a free subscription to the
Catalyst, our quarterly hardcopy newsletter, please forward your mailing address
to info@psychlaws.org.
The Center does not accept donations from pharmaceutical companies. Support
from individuals who share our mission, however, is essential to our ability to
effectively help our most vulnerable citizens. The Treatment Advocacy Center is
a 501(c)(3) not-for-profit organization. All contributions are tax-deductible
to the extent allowed by law. Donations to the Treatment Advocacy Center should
be sent to:
Treatment Advocacy Center
200 North Glebe Road, Suite 730
Arlington, VA 22203
703-294-6001 (main no.)
703-294-6010 (fax)
Wednesday, January 25, 2006
TAC Newsletter 1/20/06
ENEWS - TREATMENT ADVOCACY CENTER
TREATMENT ADVOCACY CENTER
Visit our web site www.psychlaws.org
January 20, 2006
******************************
SEATTLE POST-INTELLIGENCER, January 12, 2006
[Editor’s Note: How profoundly can the symptoms of a mental illness engulf a
person’s perceptions and rationality? – powerfully enough to make a mother take
the life of a beloved child. That point has been repeatedly reinforced in a
string of similar tragedies over the last few years, most notoriously the deaths
of Andrea Yates’ five children.
By presenting Lori Farmer ten years after her horrific event, this piece offers
a viewpoint unavailable to us in examining those more recent tragedies. She is
understandably imbued with melancholy, but she is also functional, stable and
decidedly non-violent. Her recovery leaves little doubt that her son’s life was
taken not by her but by the effects of her illness.]
TAMING A DEFIANT MIND
Lori Farmer's Recovery From Mental Illness Opens Window On Insanity Defense
By Tracy Johnson, Seattle Post-Intelligencer Reporter
Lori Farmer paces around with her guitar on open-mike night at the sandwich
shop, a colorful place filled with other eager performers who don't know about
her past.
The song she will sing mentions him, but not what happened. Not how.
She settles down at a table, sips her coffee and skims the topic, anyway.
Delving too deep, she still cries.
"I'm afraid people will persecute me. They'll say: 'Look at her. Do you know
what she did?' "
Her friend Brian Rogers tells her again. He tells her often:
"You're not the same person now."
Farmer says she knows. She was sick. The voices weren't real. God would never
urge her to hurt someone -- least of all her 4-year-old son, who loved Batman
and used to run around in a cape that his grandma made from an old skirt.
Zane was buried in his pretend cape 10 years ago. Farmer killed him.
She believed, with a rigid certainty she can still barely express, that she was
saving him. She tried to die with him. Instead, a Pierce County judge ruled her
criminally insane.
She has struggled to get hold of a defiant mind and is trying to rebuild a life.
Finding 'A Quality Life'
Farmer's story is a rare look at what happens to people who are found not guilty
by reason of insanity, sent to one of the state's two psychiatric hospitals and,
because of privacy laws, are often forgotten by the general public.
Yet of the 27 people who killed someone in Washington and were found insane
between 1995 and May 2005, 13 have already earned some degree of freedom,
according to a Seattle P-I analysis of court records, mental-health evaluations
and interviews with prosecutors and defense lawyers across the state.
Nine of them, including Farmer, have moved back into communities.
They include Bruce Rowan, a Port Angeles doctor found insane for killing his
wife with a baseball bat and an ax, and John Hallinan, who climbed into the
bathtub at a Federal Way motel six years ago and drowned his 3-year-old son.
In their cases, mental-health professionals generally found -- and judges agreed
-- that proper medication, treatment and a strong understanding of their
disorders make it unlikely they will commit another crime.
Most of the nine, like Farmer, who lives in a Lakewood group home, remain under
supervision and probably will for the rest of their lives.
Four more people, like Marc Gerson, who torched his family's Redmond home six
years ago because he thought demons told him to, have earned their way to
Western State's community program. The unlocked ward helps patients make the
transition to freedom.
The rest of the 27, like Dan Van Ho, who stabbed to death a retired Seattle
firefighter in a random attack outside the Kingdome in 1997, are still
considered unstable enough that they require 24-hour security.
Some, including Farmer, 42, may always hear voices or have delusions. The goal
of treatment, according to community program manager Dick Tomko, is to help them
find support outside the hospital's walls and "enjoy some form of a quality
life."
Early Signs Of Trouble
Years ago, Farmer's parents misread the early hints of mental illness as signs
of their daughter being a teenager.
She always thought people were looking at her and whispering behind her back.
She often seethed with anger. Her father, Deane Farmer, remembers how she
sometimes planted herself on the couch and glared at him, inexplicably fuming.
Then one day, she began screaming that demons were coming out of the bathroom
mirror at her. She started seeing "shadow people" and feeling evil spirits
brushing against her skin, crawling lightly on her arms.
She began talking about things that didn't make sense to her family. That an
unseen camera had been clicking pictures of her every move. That Jon Anderson,
lead singer of the rock group Yes, was her father in a previous life. That he
had brought her to Earth in a spaceship.
She started drinking and smoking pot. She tried to hurt herself. Her mother,
Elva Farmer, recalls finding blood-soaked tissues and questioning her daughter,
who eventually admitted she'd made cuts across her wrists.
"If I tried to talk to her about it, she'd just pick a fight about something
else," Elva said.
They knew little about mental illness and recall that it was "pretty much kicked
under the carpet" back then, she said. They sometimes wondered if Lori's odd
behavior was a ploy; it often came when she didn't get what she wanted.
Eventually, they helped her move into an apartment and supported her
financially.
"I have to confess," her mother recalled, "it was a lot easier to pay her rent
than to live with her."
Multiple Suicide Attempts
Farmer knew something was wrong. Other people didn't spend full days sobbing.
She would go to church but otherwise isolate herself in her Tacoma apartment.
She didn't have any friends. She'd sit alone and play her guitar.
Some days she felt almost normal. Some days she couldn't pull herself out of
bed.
"I felt like somebody hit my soul with a Mack truck," she recalled.
She heard angry voices, sometimes God, sometimes Satan, and started using harder
drugs such as methamphetamine. She was trying to get through the day any way she
could, thinking, "If I die, I die."
One night she cut her wrists so deeply that she almost did.
A doctor first prescribed an anti-depressant after one of her suicide attempts,
but she wouldn't always take it. She got counseling, too, but it didn't help.
Her parents say she had a way of "masquerading" -- pretending she was fine.
They wanted her to get help but couldn't force an adult who didn't want it. They
weren't allowed to see her medical records, so she was able to keep them in the
dark.
Her father recalled simply, "We didn't know what to do."
Tough Defense To Prove
Many lawyers consider insanity a defense of last resort.
Juries seldom find people insane in murder cases. It appears to have happened
just once in the past decade in Washington, in the case of Rowan, the Port
Angeles doctor. And judges, as in Farmer's case, rarely do either.
At least 3,342 people were charged with homicide in Washington between January
1994 and December 2004. Less than 1 percent of them were ruled insane.
Proving someone is not guilty by reason of insanity is tough. It's not enough
that the person is mentally ill, hears strange voices or has a long, documented
psychiatric history.
Under state law, it means a mental "disease or defect" made the person either
unable to "perceive the nature and quality" of the crime or to distinguish
between right and wrong at that time.
The "not guilty" part can be a wrenching concept for victims' relatives to
accept: that legally, no one is responsible.
"I think most of the time it's met with great skepticism because murder is a
deliberate act of one human against another," said Jenny Wieland, director of
Families and Friends of Violent Crime Victims, a Washington-based victims'
advocacy group.
But mental health advocates say delusions can obliterate a person's perception
of what is real and what is right.
They say sending such people to prison -- blaming them for their disorder
instead of treating it -- doesn't bring justice for anyone.
"There's a legitimate public interest to make sure there's no recurrence," said
Ron Honberg of the National Alliance on Mental Illness.
"Maximum-security prisons are environments that are pretty much guaranteed to
make symptoms of mental illness worse."
A Boy Called Bucky
Farmer keeps a small photo album full of pictures of Zane, who had shiny brown
hair and got a kick out of putting his hands over his eyes and hollering,
"Somebody turned out the lights!"
As she sat on a picnic bench on an outing with her Western State therapist, Kris
Harkness, her memories of Zane tumbled out. She smoked a menthol as she talked
about him with a proud smile and sad eyes.
She used to call him Bucky, and he could almost always sweet-talk her into
buying him a new toy. Once Farmer told him he had too many and should give some
to the Salvation Army. He thought about it and brought it up the next day.
"Mom, don't give all my toys to the mations!" he told her, a bizarre word that
still makes her laugh.
His father was a man Farmer had met on the psychiatric ward at a Pierce County
hospital, where she ended up after a suicide attempt in 1989, but she didn't
stay with him for long.
Farmer acknowledges now that she often wasn't a good mom. She was sick, and like
many mentally ill people, was trying to feel well by using drugs. Some mornings
Zane found her too depressed to drag herself out of bed.
"He'd say, 'Take your medication, Momma,' " Farmer recalled. "He knew."
She had been prescribed several anti-depressant and anti-psychotic drugs over
the years, but they made her feel weak and anxious and gain weight. She'd feel
drained and ugly and quit taking them, then skid toward paranoia.
Once she saw construction workers outside her apartment and became convinced
that they were nailing boards over the doors to trap her inside.
She became preoccupied with the Antichrist, the Mark of the Beast at the
Apocalypse, concepts she'd learned about in church. She worried constantly about
kidnappers and sex predators, certain that one was going to snatch Zane.
As she fought with her fears, her parents recalled, she tried to put everything
she had into taking care of Zane. That was clear to Elva Farmer even as she
cleaned out Lori's apartment after her grandson was gone.
"When I went to his little dresser, all his things were folded so neatly. His
socks were all rolled up," Elva recalled. "Everything of Lori's was just a
mess."
A Reeling Mind, A Gunshot
Farmer was expecting her parents for dinner on June 13, 1995.
Zane was playing outside while she stood at the stove, trying to make spaghetti
sauce. She couldn't concentrate. She recalls hearing the voice of God: This is
it, he told her. Suddenly, she had to get Zane.
Her mind was racing with all that was real to her: Jon Anderson, the musician,
the man who brought her to Earth in a spaceship in another life, was now the
Antichrist in this one. He was coming. The Apocalypse was at hand.
Her neighbors were in on it. Zane would be given the Mark of the Beast, and the
Antichrist would take him away. She had to make sure she and Zane went to
heaven. Together.
The meat for the spaghetti sauce burned.
Farmer hurried outside and led Zane in by the hand. He was hungry. He headed for
the pantry and rummaged around for a snack. Farmer got the gun she'd bought to
protect them some earlier time when her mind had churned out illusory reasons
for alarm.
She remembers reaching one hand to her little boy's face.
"I said, 'Zane, I love you,' " she recalled, eyes filling with the tears that
nearly always come. "And I covered his eyes so he couldn't see."
She shot him in the chest. She remembers leaning his small body over gently on
the pantry floor.
"I thought I was saving him," she said. "I believed it with all my heart."
She sprawled next to him on the floor and curled the gun around, resting the
barrel against her own chest. Fired once. Tried again.
Wounded, bleeding, she fought with the weapon. It was jammed. She felt warm; the
pain wouldn't rush in until later.
The next hours collapsed into each other. Her parents came over, knocked
repeatedly and left. Night fell. Farmer fumbled around for some knives, carved
open her wrists and lay down on her bed.
Zane was on his way to heaven. She had to catch up.
No Dispute Of Her Insanity
Farmer was inconsolable, rocking, crying. Doctors at two other hospitals had
treated the bullet wound in her chest and her sliced arms after her parents went
to her apartment and discovered what she had done.
Now sitting at Western State Hospital, she was almost unrecognizable.
"When I first saw her, I never thought she'd get well again," her mother said.
"There wasn't much to say. We just sat and cried. She said, 'I tried to save
him.' I tried to tell her, 'Well, you're still here. The end of the world hasn't
happened.' "
Farmer was charged with murder. A psychologist asked by the court to evaluate
her concluded she was legally insane when she killed her son: that while she
understood what she was doing, she couldn't tell right from wrong.
Pierce County prosecutors knew it would be difficult to prove otherwise and, in
a rare decision, agreed Farmer should be found insane, according to Jerry
Costello, chief criminal deputy prosecutor.
For many months, Farmer would "sob for extended periods throughout the day" and
had "auditory and visual hallucinations, especially of angels and other
spiritual figures," according to a hospital report.
Her parents tried to learn what they could about Farmer's mental problems, which
they found, only after Zane's death, included schizoaffective disorder --
essentially schizophrenia with shades of depression.
Hospital staff watched her carefully, wary that she might try again to kill
herself. She so urgently wanted to be with Zane.
"She said, 'I just want to die.' She said that for a good four or five years,' "
Elva Farmer recalled. "It was hideous. Just heartbreaking."
Treatment, Not Punishment
If she had been found guilty, Farmer might still be behind bars. A second-degree
murder conviction can mean 10 to 18 years in prison or longer.
To mental-health advocates, the time isn't the point. The goal isn't punishment;
it's helping people learn to manage their illness, which often takes much longer
than the sentence would have been.
"You're not sent to the state hospital to 'do time'; you're sent there to get
treatment," said Deborah Dorfman, director of legal advocacy for Washington
Protection and Advocacy System, which works to protect the rights of people with
disabilities including mental illness.
"It's not like they're discharging people right and left," she said. "Getting a
conditional release (from a psychiatric hospital) is not easy. It's not taken
lightly."
Still, some worry that the hospital staff members who recommend release -- or
the judges who agree to it -- might make mistakes in deciding whether someone
still poses a risk.
Many victims' relatives want to see mentally ill offenders locked up for more
time simply "because they committed a crime, and there's got to be
accountability," said Wieland of the victims' advocacy group.
Zane's father, Tom Dickerson, said that although he's been diagnosed with
paranoid schizophrenia himself, his understanding of mental illness doesn't calm
his anger about what Farmer did.
"I think she should have went to prison," said Dickerson, 35, who is behind bars
in Idaho for failing to register as a sex offender after a 1990 rape conviction.
"She lost a son, and I know she really loved him, but he was all I had."
Refusing Her Responsibility
As doctors searched for the right balance of anti-psychotic and anti-depressant
medications, Elva Farmer remembers, Lori became fidgety. In the first year after
the shooting, she talked more but would unconsciously stamp her feet on the
floor. She couldn't sleep.
And for a long time, Lori tried to blame others for Zane's death.
God shouldn't have let it happen, she'd tell people. The devil shouldn't have
tricked her. Her psychiatrists must have prescribed the wrong medications. Her
mother should have seen it coming.
"It was so much pain," Farmer recalled. "I had to have somewhere for it to go."
Hospital staff were gently trying to help her understand that her own actions,
while she was psychotic, led to Zane's death.
"This is a very difficult process for any patient to come to grips with," they
wrote in 1996, "as there is so much guilt."
Getting Better Was Worse
In their twice-yearly reports, hospital staff said Farmer was impulsive.
She broke rules. She traded food with a patient who was supposed to be on a
special diet. She got caught smoking in various places on the ward, lighting
cigarettes with a hairdryer.
Once, as patients were filing down a stairwell, she spontaneously yelled, "Run,
everybody, run!"
Every time she'd start to improve, earning a new level of responsibility under
the hospital's motivational system, she'd backslide.
"I think it was self-punishment," Elva Farmer said. "Her son was dead, and she
didn't think she deserved anything because of it."
Medications have a way of generating more anguish long before bringing hope.
They can expose reality.
Farmer remembers slowly realizing the Antichrist hadn't been coming for her and
Zane that day. Her mind had created this delusion. This lie. And still, Zane was
gone.
It tore at her all the time.
She hurt so many people. Her parents, who adored their grandson. His playmates.
Zane was their first friend who died and the reason they had to learn, so young,
what that meant.
"I had to face what I did," Farmer said. "It wasn't like I spilled a gallon of
milk. I mean, Zane died."
"There was a time, as she began to get better mentally, that the better she got,
the worse it was," her mother remembered. "She'd cry and cry."
'Guilty But Mentally Ill'
People have been found not guilty by reason of insanity for centuries, though
the idea has always brought controversy.
In 1982, when John Hinckley Jr. was found insane after shooting President Reagan
in an apparent attempt to impress actress Jodie Foster, many states took steps
to make it harder for mentally ill people to be acquitted.
Several states did away with the insanity defense altogether. Others gave juries
another option: a "guilty but insane" or "guilty but mentally ill" verdict. The
idea is that people will get treatment, then spend the rest of their sentence
behind bars.
Families and Friends of Violent Crime Victims plans to propose a similar law in
Washington state this year.
"The benefits would be for the victims, really," said Ida Ballasiotes, vice
chairwoman of the group's board and a former state representative. "At least
there's a little sense of closure."
The group's proposal will likely echo legislation once put forward by former
state lawmaker Jeri Costa, who now heads the state's Indeterminate Sentence
Review Board. It would let juries find people "guilty and mentally ill."
"Whether they knew what they were doing at the time or not, they killed
somebody," Costa said. "The No. 1 issue here is that there's no accountability."
Mental-heath advocates argue that such an approach has a fundamental flaw: It
means locking up people for acts prompted by illnesses that aren't their fault.
The National Alliance on Mental Illness opposes such laws because "they are used
to punish rather than treat persons with brain disorders who have committed
crimes as a consequence of their brain disorders."
Critics also contend it's just a regular guilty verdict in disguise -- with a
feel-good provision about treatment that people won't likely get because there
won't be resources to provide it.
"I think it's just something to mislead the jury," said Seattle lawyer David
Allen, who defended Rowan seven years ago. "And I don't think there's a problem
anyway, because very few juries ever acquit."
Accepting Her Illness
In her tiny room at the hospital, Farmer intermittently hung pictures of Jon
Anderson and Jesus, then ripped them down. Sometimes the images were reassuring
to see; sometimes she felt like they were saying bad things to her.
Hospital staff said her spirits could soar or crash depending on whether she
believed, at any particular time, that she and Anderson would be together in
another life.
She went to daily group therapy, where patients talked about why they needed to
be hospitalized and how to prevent relapse. She attended sessions about the
importance of medications, the side effects and the need to steer clear of
street drugs.
By 2002, she began asking more questions about her illness and had "shown desire
to understand her behavior," according to a hospital report.
She admitted the voice of Jesus had been keeping her up at night. She realized
that hiding her symptoms hadn't persuaded anyone to free her and wasn't helping
her get better.
Staff saw signs that she was beginning to accept her illness and what it would
mean for her life. She talked about a future that involved making supportive new
friends, taking medication and probably never living alone.
In early 2004, hospital staff decided she was ready -- a Pierce County Superior
Court judge agreed -- to move to the community program.
There, she was gradually allowed to leave the hospital grounds -- at first for
an hour, eventually for weekend furloughs when she'd sometimes go camping with
her parents -- as she worked toward freedom.
Low Rate Of Reoffending
Some of the people who have committed crimes and live in Western State
Hospital's locked ward don't want help. They resent supervision. They don't
believe they are sick or try to pretend they aren't.
"Some people continue to blame other people or don't want to deal with the
seriousness of their crime," said Tomko, the community program manager. "Those
are the people who don't get out."
Yet patients don't have to show they are somehow "cured" to be released; it's a
matter of whether they are considered at risk of breaking the law again. They
must also show they can keep their symptoms in check.
Whether someone should move to the unlocked community program or into society is
up to the hospital's risk-review board, which also considers the patient's
attitude toward treatment, plan for the future and support outside the hospital.
People who are treated at places such as Western State Hospital are much less
likely to commit another crime than those who land in prison, according to Bruce
Gage, supervising psychiatrist for the hospital's Center for Forensic Services.
He said most people released from prison will break the law within three years,
while the recidivism rate for people found insane and treated at a specialized
psychiatric program is less than 5 percent.
Dealing With The Voices
Farmer now wants to understand as much as she can about the mental disorder she
used to pretend wasn't there. She wants to retain control of it.
"She's very genuine; very honest," said her therapist, Harkness, whom Farmer
calls her guardian angel. "She'll tell you when she has symptoms. She wants
help."
Despite her medication, the voices are still there occasionally. They don't
command her to do anything, which hospital staff would find more troubling.
She sometimes hears Jesus, God or even Anderson, whom she still believes was her
father in a previous life but now realizes isn't the Antichrist. They say
negative things, that they're going to punish her, make her fat, make her hair
fall out.
Jesus tells her, "Woe to you."
Sometimes she ignores the voices. Sometimes they grow too loud.
Then Farmer gets what she calls "a reality check" to help make sure these
hallucinations never again whirl out of control. She'll ask her mom, Harkness or
whoever is around: Could the voices be real?
Harkness sometimes tells Farmer to try to shut the voices out. They are her
illness. Her mom explains that God and Jesus are loving. They wouldn't want to
punish her.
Farmer said she thinks about it for a while, follows the logic, "and then I
start reasoning right."
Support Makes A Difference
At the end of August, Farmer moved off the campus of Western State and into a
group home, which has about 20 other residents and staff who work there full
time.
Harkness continues to see her at least weekly to talk about her symptoms,
budgeting her limited Social Security money -- most of it goes to the group home
-- or whatever else comes up.
At some point, Farmer plans to look for a job, maybe in a mailroom somewhere,
with very limited hours to curb potential stress.
Every Wednesday, she goes to a group session about substance abuse at Greater
Lakes Mental Healthcare, where she has a case manager and someone who prescribes
her medication.
She likes to relax at her parents' cheery rambler in Sumner. Her mom and dad
have given her constant support over the years, according to hospital reports --
often a powerful part of a patient's recovery.
Her mother said she misses her grandson but has never felt like she couldn't
forgive her daughter.
"We lost one to this illness," she said. "There's no point in losing two."
Farmer often talks about how she'll always have to take medications and will
never again drink alcohol or do street drugs. If she does, or if her mental
illness otherwise grows worse, Western State staff can bring her right back to
the hospital.
A Pierce County judge also reviews hospital reports about Farmer, sent at least
twice a year, to consider how she's doing and whether there's any reason she
shouldn't remain free.
Farmer said she now wants to keep other mentally ill people from ending up in
her situation. To keep taking their medication. To realize that they can't
simply ignore what's going on in their heads.
She has seen her own illness at its worst and must live with the consequences.
"I want to see me make it, and I'm going to," she said. "I don't want to hurt
anybody. I don't want to hurt myself. I want to have a peaceful, successful life
now."
Her Radiant Star
Farmer waits for her turn to sing at the Antique Sandwich Co. in Tacoma. She's
wearing a new outfit and an elaborate necklace jeweled with colored stones.
She shows off the brown felt hat she's brought with her. Should she wear it or
not? She asks a few people. She puts it on. She takes it off. She declares, "I'm
not nervous at all."
On stage, she begins strumming her guitar, her thick silver rings flashing, her
short, sapphire-painted fingernails finding the chords. She's playing "Radiant
Star," a song she's written about Jesus being there during her toughest times.
I got drunk at the bar; I slept in my car, she begins, her voice deep and
strong. But you were my radiant star.
She closes her eyes, moving to the music. My son died one day; in heaven he
plays. But you are my radiant star.
Sometimes she sings "Zane's Song." That one's harder.
Maybe she'll play it next time.
******************************
Treatment Advocacy Center E-NEWS is a publication of the Treatment Advocacy
Center.
This E-NEWS is provided as a public service by the Treatment Advocacy Center.
There is no fee. If you would also like to receive a free subscription to the
Catalyst, our quarterly hardcopy newsletter, please forward your mailing address
to info@psychlaws.org.
The Center does not accept donations from pharmaceutical companies. Support
from individuals who share our mission, however, is essential to our ability to
effectively help our most vulnerable citizens. The Treatment Advocacy Center is
a 501(c)(3) not-for-profit organization. All contributions are tax-deductible
to the extent allowed by law. Donations to the Treatment Advocacy Center should
be sent to:
Treatment Advocacy Center
200 North Glebe Road, Suite 730
Arlington, VA 22203
703-294-6001 (main no.)
703-294-6010 (fax)
TREATMENT ADVOCACY CENTER
Visit our web site www.psychlaws.org
January 20, 2006
******************************
SEATTLE POST-INTELLIGENCER, January 12, 2006
[Editor’s Note: How profoundly can the symptoms of a mental illness engulf a
person’s perceptions and rationality? – powerfully enough to make a mother take
the life of a beloved child. That point has been repeatedly reinforced in a
string of similar tragedies over the last few years, most notoriously the deaths
of Andrea Yates’ five children.
By presenting Lori Farmer ten years after her horrific event, this piece offers
a viewpoint unavailable to us in examining those more recent tragedies. She is
understandably imbued with melancholy, but she is also functional, stable and
decidedly non-violent. Her recovery leaves little doubt that her son’s life was
taken not by her but by the effects of her illness.]
TAMING A DEFIANT MIND
Lori Farmer's Recovery From Mental Illness Opens Window On Insanity Defense
By Tracy Johnson, Seattle Post-Intelligencer Reporter
Lori Farmer paces around with her guitar on open-mike night at the sandwich
shop, a colorful place filled with other eager performers who don't know about
her past.
The song she will sing mentions him, but not what happened. Not how.
She settles down at a table, sips her coffee and skims the topic, anyway.
Delving too deep, she still cries.
"I'm afraid people will persecute me. They'll say: 'Look at her. Do you know
what she did?' "
Her friend Brian Rogers tells her again. He tells her often:
"You're not the same person now."
Farmer says she knows. She was sick. The voices weren't real. God would never
urge her to hurt someone -- least of all her 4-year-old son, who loved Batman
and used to run around in a cape that his grandma made from an old skirt.
Zane was buried in his pretend cape 10 years ago. Farmer killed him.
She believed, with a rigid certainty she can still barely express, that she was
saving him. She tried to die with him. Instead, a Pierce County judge ruled her
criminally insane.
She has struggled to get hold of a defiant mind and is trying to rebuild a life.
Finding 'A Quality Life'
Farmer's story is a rare look at what happens to people who are found not guilty
by reason of insanity, sent to one of the state's two psychiatric hospitals and,
because of privacy laws, are often forgotten by the general public.
Yet of the 27 people who killed someone in Washington and were found insane
between 1995 and May 2005, 13 have already earned some degree of freedom,
according to a Seattle P-I analysis of court records, mental-health evaluations
and interviews with prosecutors and defense lawyers across the state.
Nine of them, including Farmer, have moved back into communities.
They include Bruce Rowan, a Port Angeles doctor found insane for killing his
wife with a baseball bat and an ax, and John Hallinan, who climbed into the
bathtub at a Federal Way motel six years ago and drowned his 3-year-old son.
In their cases, mental-health professionals generally found -- and judges agreed
-- that proper medication, treatment and a strong understanding of their
disorders make it unlikely they will commit another crime.
Most of the nine, like Farmer, who lives in a Lakewood group home, remain under
supervision and probably will for the rest of their lives.
Four more people, like Marc Gerson, who torched his family's Redmond home six
years ago because he thought demons told him to, have earned their way to
Western State's community program. The unlocked ward helps patients make the
transition to freedom.
The rest of the 27, like Dan Van Ho, who stabbed to death a retired Seattle
firefighter in a random attack outside the Kingdome in 1997, are still
considered unstable enough that they require 24-hour security.
Some, including Farmer, 42, may always hear voices or have delusions. The goal
of treatment, according to community program manager Dick Tomko, is to help them
find support outside the hospital's walls and "enjoy some form of a quality
life."
Early Signs Of Trouble
Years ago, Farmer's parents misread the early hints of mental illness as signs
of their daughter being a teenager.
She always thought people were looking at her and whispering behind her back.
She often seethed with anger. Her father, Deane Farmer, remembers how she
sometimes planted herself on the couch and glared at him, inexplicably fuming.
Then one day, she began screaming that demons were coming out of the bathroom
mirror at her. She started seeing "shadow people" and feeling evil spirits
brushing against her skin, crawling lightly on her arms.
She began talking about things that didn't make sense to her family. That an
unseen camera had been clicking pictures of her every move. That Jon Anderson,
lead singer of the rock group Yes, was her father in a previous life. That he
had brought her to Earth in a spaceship.
She started drinking and smoking pot. She tried to hurt herself. Her mother,
Elva Farmer, recalls finding blood-soaked tissues and questioning her daughter,
who eventually admitted she'd made cuts across her wrists.
"If I tried to talk to her about it, she'd just pick a fight about something
else," Elva said.
They knew little about mental illness and recall that it was "pretty much kicked
under the carpet" back then, she said. They sometimes wondered if Lori's odd
behavior was a ploy; it often came when she didn't get what she wanted.
Eventually, they helped her move into an apartment and supported her
financially.
"I have to confess," her mother recalled, "it was a lot easier to pay her rent
than to live with her."
Multiple Suicide Attempts
Farmer knew something was wrong. Other people didn't spend full days sobbing.
She would go to church but otherwise isolate herself in her Tacoma apartment.
She didn't have any friends. She'd sit alone and play her guitar.
Some days she felt almost normal. Some days she couldn't pull herself out of
bed.
"I felt like somebody hit my soul with a Mack truck," she recalled.
She heard angry voices, sometimes God, sometimes Satan, and started using harder
drugs such as methamphetamine. She was trying to get through the day any way she
could, thinking, "If I die, I die."
One night she cut her wrists so deeply that she almost did.
A doctor first prescribed an anti-depressant after one of her suicide attempts,
but she wouldn't always take it. She got counseling, too, but it didn't help.
Her parents say she had a way of "masquerading" -- pretending she was fine.
They wanted her to get help but couldn't force an adult who didn't want it. They
weren't allowed to see her medical records, so she was able to keep them in the
dark.
Her father recalled simply, "We didn't know what to do."
Tough Defense To Prove
Many lawyers consider insanity a defense of last resort.
Juries seldom find people insane in murder cases. It appears to have happened
just once in the past decade in Washington, in the case of Rowan, the Port
Angeles doctor. And judges, as in Farmer's case, rarely do either.
At least 3,342 people were charged with homicide in Washington between January
1994 and December 2004. Less than 1 percent of them were ruled insane.
Proving someone is not guilty by reason of insanity is tough. It's not enough
that the person is mentally ill, hears strange voices or has a long, documented
psychiatric history.
Under state law, it means a mental "disease or defect" made the person either
unable to "perceive the nature and quality" of the crime or to distinguish
between right and wrong at that time.
The "not guilty" part can be a wrenching concept for victims' relatives to
accept: that legally, no one is responsible.
"I think most of the time it's met with great skepticism because murder is a
deliberate act of one human against another," said Jenny Wieland, director of
Families and Friends of Violent Crime Victims, a Washington-based victims'
advocacy group.
But mental health advocates say delusions can obliterate a person's perception
of what is real and what is right.
They say sending such people to prison -- blaming them for their disorder
instead of treating it -- doesn't bring justice for anyone.
"There's a legitimate public interest to make sure there's no recurrence," said
Ron Honberg of the National Alliance on Mental Illness.
"Maximum-security prisons are environments that are pretty much guaranteed to
make symptoms of mental illness worse."
A Boy Called Bucky
Farmer keeps a small photo album full of pictures of Zane, who had shiny brown
hair and got a kick out of putting his hands over his eyes and hollering,
"Somebody turned out the lights!"
As she sat on a picnic bench on an outing with her Western State therapist, Kris
Harkness, her memories of Zane tumbled out. She smoked a menthol as she talked
about him with a proud smile and sad eyes.
She used to call him Bucky, and he could almost always sweet-talk her into
buying him a new toy. Once Farmer told him he had too many and should give some
to the Salvation Army. He thought about it and brought it up the next day.
"Mom, don't give all my toys to the mations!" he told her, a bizarre word that
still makes her laugh.
His father was a man Farmer had met on the psychiatric ward at a Pierce County
hospital, where she ended up after a suicide attempt in 1989, but she didn't
stay with him for long.
Farmer acknowledges now that she often wasn't a good mom. She was sick, and like
many mentally ill people, was trying to feel well by using drugs. Some mornings
Zane found her too depressed to drag herself out of bed.
"He'd say, 'Take your medication, Momma,' " Farmer recalled. "He knew."
She had been prescribed several anti-depressant and anti-psychotic drugs over
the years, but they made her feel weak and anxious and gain weight. She'd feel
drained and ugly and quit taking them, then skid toward paranoia.
Once she saw construction workers outside her apartment and became convinced
that they were nailing boards over the doors to trap her inside.
She became preoccupied with the Antichrist, the Mark of the Beast at the
Apocalypse, concepts she'd learned about in church. She worried constantly about
kidnappers and sex predators, certain that one was going to snatch Zane.
As she fought with her fears, her parents recalled, she tried to put everything
she had into taking care of Zane. That was clear to Elva Farmer even as she
cleaned out Lori's apartment after her grandson was gone.
"When I went to his little dresser, all his things were folded so neatly. His
socks were all rolled up," Elva recalled. "Everything of Lori's was just a
mess."
A Reeling Mind, A Gunshot
Farmer was expecting her parents for dinner on June 13, 1995.
Zane was playing outside while she stood at the stove, trying to make spaghetti
sauce. She couldn't concentrate. She recalls hearing the voice of God: This is
it, he told her. Suddenly, she had to get Zane.
Her mind was racing with all that was real to her: Jon Anderson, the musician,
the man who brought her to Earth in a spaceship in another life, was now the
Antichrist in this one. He was coming. The Apocalypse was at hand.
Her neighbors were in on it. Zane would be given the Mark of the Beast, and the
Antichrist would take him away. She had to make sure she and Zane went to
heaven. Together.
The meat for the spaghetti sauce burned.
Farmer hurried outside and led Zane in by the hand. He was hungry. He headed for
the pantry and rummaged around for a snack. Farmer got the gun she'd bought to
protect them some earlier time when her mind had churned out illusory reasons
for alarm.
She remembers reaching one hand to her little boy's face.
"I said, 'Zane, I love you,' " she recalled, eyes filling with the tears that
nearly always come. "And I covered his eyes so he couldn't see."
She shot him in the chest. She remembers leaning his small body over gently on
the pantry floor.
"I thought I was saving him," she said. "I believed it with all my heart."
She sprawled next to him on the floor and curled the gun around, resting the
barrel against her own chest. Fired once. Tried again.
Wounded, bleeding, she fought with the weapon. It was jammed. She felt warm; the
pain wouldn't rush in until later.
The next hours collapsed into each other. Her parents came over, knocked
repeatedly and left. Night fell. Farmer fumbled around for some knives, carved
open her wrists and lay down on her bed.
Zane was on his way to heaven. She had to catch up.
No Dispute Of Her Insanity
Farmer was inconsolable, rocking, crying. Doctors at two other hospitals had
treated the bullet wound in her chest and her sliced arms after her parents went
to her apartment and discovered what she had done.
Now sitting at Western State Hospital, she was almost unrecognizable.
"When I first saw her, I never thought she'd get well again," her mother said.
"There wasn't much to say. We just sat and cried. She said, 'I tried to save
him.' I tried to tell her, 'Well, you're still here. The end of the world hasn't
happened.' "
Farmer was charged with murder. A psychologist asked by the court to evaluate
her concluded she was legally insane when she killed her son: that while she
understood what she was doing, she couldn't tell right from wrong.
Pierce County prosecutors knew it would be difficult to prove otherwise and, in
a rare decision, agreed Farmer should be found insane, according to Jerry
Costello, chief criminal deputy prosecutor.
For many months, Farmer would "sob for extended periods throughout the day" and
had "auditory and visual hallucinations, especially of angels and other
spiritual figures," according to a hospital report.
Her parents tried to learn what they could about Farmer's mental problems, which
they found, only after Zane's death, included schizoaffective disorder --
essentially schizophrenia with shades of depression.
Hospital staff watched her carefully, wary that she might try again to kill
herself. She so urgently wanted to be with Zane.
"She said, 'I just want to die.' She said that for a good four or five years,' "
Elva Farmer recalled. "It was hideous. Just heartbreaking."
Treatment, Not Punishment
If she had been found guilty, Farmer might still be behind bars. A second-degree
murder conviction can mean 10 to 18 years in prison or longer.
To mental-health advocates, the time isn't the point. The goal isn't punishment;
it's helping people learn to manage their illness, which often takes much longer
than the sentence would have been.
"You're not sent to the state hospital to 'do time'; you're sent there to get
treatment," said Deborah Dorfman, director of legal advocacy for Washington
Protection and Advocacy System, which works to protect the rights of people with
disabilities including mental illness.
"It's not like they're discharging people right and left," she said. "Getting a
conditional release (from a psychiatric hospital) is not easy. It's not taken
lightly."
Still, some worry that the hospital staff members who recommend release -- or
the judges who agree to it -- might make mistakes in deciding whether someone
still poses a risk.
Many victims' relatives want to see mentally ill offenders locked up for more
time simply "because they committed a crime, and there's got to be
accountability," said Wieland of the victims' advocacy group.
Zane's father, Tom Dickerson, said that although he's been diagnosed with
paranoid schizophrenia himself, his understanding of mental illness doesn't calm
his anger about what Farmer did.
"I think she should have went to prison," said Dickerson, 35, who is behind bars
in Idaho for failing to register as a sex offender after a 1990 rape conviction.
"She lost a son, and I know she really loved him, but he was all I had."
Refusing Her Responsibility
As doctors searched for the right balance of anti-psychotic and anti-depressant
medications, Elva Farmer remembers, Lori became fidgety. In the first year after
the shooting, she talked more but would unconsciously stamp her feet on the
floor. She couldn't sleep.
And for a long time, Lori tried to blame others for Zane's death.
God shouldn't have let it happen, she'd tell people. The devil shouldn't have
tricked her. Her psychiatrists must have prescribed the wrong medications. Her
mother should have seen it coming.
"It was so much pain," Farmer recalled. "I had to have somewhere for it to go."
Hospital staff were gently trying to help her understand that her own actions,
while she was psychotic, led to Zane's death.
"This is a very difficult process for any patient to come to grips with," they
wrote in 1996, "as there is so much guilt."
Getting Better Was Worse
In their twice-yearly reports, hospital staff said Farmer was impulsive.
She broke rules. She traded food with a patient who was supposed to be on a
special diet. She got caught smoking in various places on the ward, lighting
cigarettes with a hairdryer.
Once, as patients were filing down a stairwell, she spontaneously yelled, "Run,
everybody, run!"
Every time she'd start to improve, earning a new level of responsibility under
the hospital's motivational system, she'd backslide.
"I think it was self-punishment," Elva Farmer said. "Her son was dead, and she
didn't think she deserved anything because of it."
Medications have a way of generating more anguish long before bringing hope.
They can expose reality.
Farmer remembers slowly realizing the Antichrist hadn't been coming for her and
Zane that day. Her mind had created this delusion. This lie. And still, Zane was
gone.
It tore at her all the time.
She hurt so many people. Her parents, who adored their grandson. His playmates.
Zane was their first friend who died and the reason they had to learn, so young,
what that meant.
"I had to face what I did," Farmer said. "It wasn't like I spilled a gallon of
milk. I mean, Zane died."
"There was a time, as she began to get better mentally, that the better she got,
the worse it was," her mother remembered. "She'd cry and cry."
'Guilty But Mentally Ill'
People have been found not guilty by reason of insanity for centuries, though
the idea has always brought controversy.
In 1982, when John Hinckley Jr. was found insane after shooting President Reagan
in an apparent attempt to impress actress Jodie Foster, many states took steps
to make it harder for mentally ill people to be acquitted.
Several states did away with the insanity defense altogether. Others gave juries
another option: a "guilty but insane" or "guilty but mentally ill" verdict. The
idea is that people will get treatment, then spend the rest of their sentence
behind bars.
Families and Friends of Violent Crime Victims plans to propose a similar law in
Washington state this year.
"The benefits would be for the victims, really," said Ida Ballasiotes, vice
chairwoman of the group's board and a former state representative. "At least
there's a little sense of closure."
The group's proposal will likely echo legislation once put forward by former
state lawmaker Jeri Costa, who now heads the state's Indeterminate Sentence
Review Board. It would let juries find people "guilty and mentally ill."
"Whether they knew what they were doing at the time or not, they killed
somebody," Costa said. "The No. 1 issue here is that there's no accountability."
Mental-heath advocates argue that such an approach has a fundamental flaw: It
means locking up people for acts prompted by illnesses that aren't their fault.
The National Alliance on Mental Illness opposes such laws because "they are used
to punish rather than treat persons with brain disorders who have committed
crimes as a consequence of their brain disorders."
Critics also contend it's just a regular guilty verdict in disguise -- with a
feel-good provision about treatment that people won't likely get because there
won't be resources to provide it.
"I think it's just something to mislead the jury," said Seattle lawyer David
Allen, who defended Rowan seven years ago. "And I don't think there's a problem
anyway, because very few juries ever acquit."
Accepting Her Illness
In her tiny room at the hospital, Farmer intermittently hung pictures of Jon
Anderson and Jesus, then ripped them down. Sometimes the images were reassuring
to see; sometimes she felt like they were saying bad things to her.
Hospital staff said her spirits could soar or crash depending on whether she
believed, at any particular time, that she and Anderson would be together in
another life.
She went to daily group therapy, where patients talked about why they needed to
be hospitalized and how to prevent relapse. She attended sessions about the
importance of medications, the side effects and the need to steer clear of
street drugs.
By 2002, she began asking more questions about her illness and had "shown desire
to understand her behavior," according to a hospital report.
She admitted the voice of Jesus had been keeping her up at night. She realized
that hiding her symptoms hadn't persuaded anyone to free her and wasn't helping
her get better.
Staff saw signs that she was beginning to accept her illness and what it would
mean for her life. She talked about a future that involved making supportive new
friends, taking medication and probably never living alone.
In early 2004, hospital staff decided she was ready -- a Pierce County Superior
Court judge agreed -- to move to the community program.
There, she was gradually allowed to leave the hospital grounds -- at first for
an hour, eventually for weekend furloughs when she'd sometimes go camping with
her parents -- as she worked toward freedom.
Low Rate Of Reoffending
Some of the people who have committed crimes and live in Western State
Hospital's locked ward don't want help. They resent supervision. They don't
believe they are sick or try to pretend they aren't.
"Some people continue to blame other people or don't want to deal with the
seriousness of their crime," said Tomko, the community program manager. "Those
are the people who don't get out."
Yet patients don't have to show they are somehow "cured" to be released; it's a
matter of whether they are considered at risk of breaking the law again. They
must also show they can keep their symptoms in check.
Whether someone should move to the unlocked community program or into society is
up to the hospital's risk-review board, which also considers the patient's
attitude toward treatment, plan for the future and support outside the hospital.
People who are treated at places such as Western State Hospital are much less
likely to commit another crime than those who land in prison, according to Bruce
Gage, supervising psychiatrist for the hospital's Center for Forensic Services.
He said most people released from prison will break the law within three years,
while the recidivism rate for people found insane and treated at a specialized
psychiatric program is less than 5 percent.
Dealing With The Voices
Farmer now wants to understand as much as she can about the mental disorder she
used to pretend wasn't there. She wants to retain control of it.
"She's very genuine; very honest," said her therapist, Harkness, whom Farmer
calls her guardian angel. "She'll tell you when she has symptoms. She wants
help."
Despite her medication, the voices are still there occasionally. They don't
command her to do anything, which hospital staff would find more troubling.
She sometimes hears Jesus, God or even Anderson, whom she still believes was her
father in a previous life but now realizes isn't the Antichrist. They say
negative things, that they're going to punish her, make her fat, make her hair
fall out.
Jesus tells her, "Woe to you."
Sometimes she ignores the voices. Sometimes they grow too loud.
Then Farmer gets what she calls "a reality check" to help make sure these
hallucinations never again whirl out of control. She'll ask her mom, Harkness or
whoever is around: Could the voices be real?
Harkness sometimes tells Farmer to try to shut the voices out. They are her
illness. Her mom explains that God and Jesus are loving. They wouldn't want to
punish her.
Farmer said she thinks about it for a while, follows the logic, "and then I
start reasoning right."
Support Makes A Difference
At the end of August, Farmer moved off the campus of Western State and into a
group home, which has about 20 other residents and staff who work there full
time.
Harkness continues to see her at least weekly to talk about her symptoms,
budgeting her limited Social Security money -- most of it goes to the group home
-- or whatever else comes up.
At some point, Farmer plans to look for a job, maybe in a mailroom somewhere,
with very limited hours to curb potential stress.
Every Wednesday, she goes to a group session about substance abuse at Greater
Lakes Mental Healthcare, where she has a case manager and someone who prescribes
her medication.
She likes to relax at her parents' cheery rambler in Sumner. Her mom and dad
have given her constant support over the years, according to hospital reports --
often a powerful part of a patient's recovery.
Her mother said she misses her grandson but has never felt like she couldn't
forgive her daughter.
"We lost one to this illness," she said. "There's no point in losing two."
Farmer often talks about how she'll always have to take medications and will
never again drink alcohol or do street drugs. If she does, or if her mental
illness otherwise grows worse, Western State staff can bring her right back to
the hospital.
A Pierce County judge also reviews hospital reports about Farmer, sent at least
twice a year, to consider how she's doing and whether there's any reason she
shouldn't remain free.
Farmer said she now wants to keep other mentally ill people from ending up in
her situation. To keep taking their medication. To realize that they can't
simply ignore what's going on in their heads.
She has seen her own illness at its worst and must live with the consequences.
"I want to see me make it, and I'm going to," she said. "I don't want to hurt
anybody. I don't want to hurt myself. I want to have a peaceful, successful life
now."
Her Radiant Star
Farmer waits for her turn to sing at the Antique Sandwich Co. in Tacoma. She's
wearing a new outfit and an elaborate necklace jeweled with colored stones.
She shows off the brown felt hat she's brought with her. Should she wear it or
not? She asks a few people. She puts it on. She takes it off. She declares, "I'm
not nervous at all."
On stage, she begins strumming her guitar, her thick silver rings flashing, her
short, sapphire-painted fingernails finding the chords. She's playing "Radiant
Star," a song she's written about Jesus being there during her toughest times.
I got drunk at the bar; I slept in my car, she begins, her voice deep and
strong. But you were my radiant star.
She closes her eyes, moving to the music. My son died one day; in heaven he
plays. But you are my radiant star.
Sometimes she sings "Zane's Song." That one's harder.
Maybe she'll play it next time.
******************************
Treatment Advocacy Center E-NEWS is a publication of the Treatment Advocacy
Center.
This E-NEWS is provided as a public service by the Treatment Advocacy Center.
There is no fee. If you would also like to receive a free subscription to the
Catalyst, our quarterly hardcopy newsletter, please forward your mailing address
to info@psychlaws.org.
The Center does not accept donations from pharmaceutical companies. Support
from individuals who share our mission, however, is essential to our ability to
effectively help our most vulnerable citizens. The Treatment Advocacy Center is
a 501(c)(3) not-for-profit organization. All contributions are tax-deductible
to the extent allowed by law. Donations to the Treatment Advocacy Center should
be sent to:
Treatment Advocacy Center
200 North Glebe Road, Suite 730
Arlington, VA 22203
703-294-6001 (main no.)
703-294-6010 (fax)
Saturday, January 21, 2006
Kendra's Law in New York
Read about it here.
Who may be affected by Kendra's Law?
A person may be ordered to obtain Assisted Outpatient Treatment (AOT) if the court finds that he or she:
is at least 18 years of age and suffers from a mental illness; and
is unlikely to survive in the community without supervision, based on a clinical determination; and
has a history of non-compliance with treatment for mental illness which has led to either 2 hospitalizations for mental illness in the preceding 3 years, or resulted in at least 1 act of violence toward self or others, or threats of serious physical harm to self or others, within the preceding 4 years; and
is unlikely to accept the treatment recommended in the treatment plan; and
is in need of AOT to avoid a relapse or deterioration that would likely result in serious harm to self or others; and
will likely benefit from AOT.
Before a court may order AOT, it must be satisfied that AOT is the least restrictive alternative for the person. Thus, if a less restrictive program or treatment exists that could effectively deal with the person's mental illness, the court will not issue an order for assisted outpatient treatment.
Whom should I contact if I think someone needs assistance through AOT?
Contact your county (or City of New York) mental health director. (A list of telephone numbers for New York State county mental health agencies can be found here.) He/she is responsible for operating the county's AOT program, and can help you determine if the person meets the criteria for AOT. He/she may also be aware of other available services if AOT is not appropriate for the individual.
What is the process to get AOT for someone?
The first step is filing a petition with the county court or supreme court for the county where the person is present or is believed to be present. People authorized to file petitions for AOT are:
a parent, spouse, adult sibling or adult child of the person;
an adult roommate;
the director of a hospital in which the person is hospitalized
the director of an organization, agency or home in which the person resides and receives mental health services;
a psychiatrist who is either treating or supervising the person's treatment;
the mental health director or social services official for the county (or City of New York) where the person is believed to be present;
a parole or probation officer assigned to supervise the person.
What specifically needs to be filed with the court to begin the process?
The petition, which is a formal statement of facts demonstrating that the person meets the criteria for AOT, must be accompanied by the affidavit of an examining physician. The affidavit must show that the physician examined the person within 10 days of the filing of the petition, and that he or she meets the criteria for AOT. If the subject of the petition has refused examination, the physician's affidavit must state that attempts at examination were made and that the physician believes the individual meets the AOT criteria. Several other procedural forms must also be filed, and standard fees must be paid at the time of filing. All necessary forms are available through your county mental health department.
Does anything else need to be done?
Once the petition is filed with the court, copies must be served on:
the person who is the subject of the petition;
Mental Hygiene Legal Service;
any health care agent appointed by the person in a health care proxy, if known;
the Program Coordinator appointed by the New York State Office of Mental Health to oversee local AOT programs; and
the appropriate county (or City of New York) mental health director.
What happens next?
The court is required to set a hearing date that is no more than 3 days after the court receives the petition. (The hearing may be adjourned to a later date if the court finds good cause for doing so.) At the hearing, the court will hear testimony of the physician whose affidavit was filed with the petition, and may also consider testimony of the petitioner and the subject of the petition. Other forms of admissible evidence may be considered as well. If the court determines by clear and convincing evidence that the criteria for AOT are met, and a written treatment plan has been filed with the court, an order for assisted outpatient treatment is issued.
To whom is the court order directed?
The court order is directed to both the person receiving AOT and the local director of the AOT program. The order will require the person to accept the treatment deemed necessary by the court, and will require the local director to furnish such treatment.
How long does the person remain in the AOT program?
The initial court order is effective for up to 6 months from the date of the order. The order can be extended for successive periods of up to 1 year each, but any application to extend AOT requires a showing that the person continues to meet all of the AOT criteria.
What happens if the person does not comply with the terms of the court order?
If a physician determines that the person may need involuntary admission to a hospital, the physician may recommend that the person be transported to a hospital and retained for up to 72 hours to determine if inpatient care and treatment are necessary. Any refusal of the person to take prescribed medication, or the failure of a test to determine either medication compliance or alcohol or drug use, may be considered by the physician in reaching the clinical determination regarding involuntary admission. Any decision to retain the person beyond the initial 72 hours must be in accordance with the procedures for involuntary admission set forth in Mental Hygiene Law.
Whom do I contact if I have additional questions about assisted outpatient treatment?
Contact your county (or City of New York) mental health director for further information. A list of telephone numbers for New York State county mental health agencies can be found here.
Who may be affected by Kendra's Law?
A person may be ordered to obtain Assisted Outpatient Treatment (AOT) if the court finds that he or she:
is at least 18 years of age and suffers from a mental illness; and
is unlikely to survive in the community without supervision, based on a clinical determination; and
has a history of non-compliance with treatment for mental illness which has led to either 2 hospitalizations for mental illness in the preceding 3 years, or resulted in at least 1 act of violence toward self or others, or threats of serious physical harm to self or others, within the preceding 4 years; and
is unlikely to accept the treatment recommended in the treatment plan; and
is in need of AOT to avoid a relapse or deterioration that would likely result in serious harm to self or others; and
will likely benefit from AOT.
Before a court may order AOT, it must be satisfied that AOT is the least restrictive alternative for the person. Thus, if a less restrictive program or treatment exists that could effectively deal with the person's mental illness, the court will not issue an order for assisted outpatient treatment.
Whom should I contact if I think someone needs assistance through AOT?
Contact your county (or City of New York) mental health director. (A list of telephone numbers for New York State county mental health agencies can be found here.) He/she is responsible for operating the county's AOT program, and can help you determine if the person meets the criteria for AOT. He/she may also be aware of other available services if AOT is not appropriate for the individual.
What is the process to get AOT for someone?
The first step is filing a petition with the county court or supreme court for the county where the person is present or is believed to be present. People authorized to file petitions for AOT are:
a parent, spouse, adult sibling or adult child of the person;
an adult roommate;
the director of a hospital in which the person is hospitalized
the director of an organization, agency or home in which the person resides and receives mental health services;
a psychiatrist who is either treating or supervising the person's treatment;
the mental health director or social services official for the county (or City of New York) where the person is believed to be present;
a parole or probation officer assigned to supervise the person.
What specifically needs to be filed with the court to begin the process?
The petition, which is a formal statement of facts demonstrating that the person meets the criteria for AOT, must be accompanied by the affidavit of an examining physician. The affidavit must show that the physician examined the person within 10 days of the filing of the petition, and that he or she meets the criteria for AOT. If the subject of the petition has refused examination, the physician's affidavit must state that attempts at examination were made and that the physician believes the individual meets the AOT criteria. Several other procedural forms must also be filed, and standard fees must be paid at the time of filing. All necessary forms are available through your county mental health department.
Does anything else need to be done?
Once the petition is filed with the court, copies must be served on:
the person who is the subject of the petition;
Mental Hygiene Legal Service;
any health care agent appointed by the person in a health care proxy, if known;
the Program Coordinator appointed by the New York State Office of Mental Health to oversee local AOT programs; and
the appropriate county (or City of New York) mental health director.
What happens next?
The court is required to set a hearing date that is no more than 3 days after the court receives the petition. (The hearing may be adjourned to a later date if the court finds good cause for doing so.) At the hearing, the court will hear testimony of the physician whose affidavit was filed with the petition, and may also consider testimony of the petitioner and the subject of the petition. Other forms of admissible evidence may be considered as well. If the court determines by clear and convincing evidence that the criteria for AOT are met, and a written treatment plan has been filed with the court, an order for assisted outpatient treatment is issued.
To whom is the court order directed?
The court order is directed to both the person receiving AOT and the local director of the AOT program. The order will require the person to accept the treatment deemed necessary by the court, and will require the local director to furnish such treatment.
How long does the person remain in the AOT program?
The initial court order is effective for up to 6 months from the date of the order. The order can be extended for successive periods of up to 1 year each, but any application to extend AOT requires a showing that the person continues to meet all of the AOT criteria.
What happens if the person does not comply with the terms of the court order?
If a physician determines that the person may need involuntary admission to a hospital, the physician may recommend that the person be transported to a hospital and retained for up to 72 hours to determine if inpatient care and treatment are necessary. Any refusal of the person to take prescribed medication, or the failure of a test to determine either medication compliance or alcohol or drug use, may be considered by the physician in reaching the clinical determination regarding involuntary admission. Any decision to retain the person beyond the initial 72 hours must be in accordance with the procedures for involuntary admission set forth in Mental Hygiene Law.
Whom do I contact if I have additional questions about assisted outpatient treatment?
Contact your county (or City of New York) mental health director for further information. A list of telephone numbers for New York State county mental health agencies can be found here.
Monday, January 16, 2006
Jim Frank, Attorney, Advocates for the Mentally Ill
State, judge clash over patient
Drug was ordered for schizophrenia, but agency contends it is too costly.
By Janet E. Williams
STAR STAFF WRITER
The Indianapolis Star
B.W.s best hope for overcoming the crippling symptoms of schizophrenia and living outside Central State Hospital is a relatively new drug called Clozaril.
So far, the price tag has kept the anti-psychotic drug beyond his reach. Clozaril costs several times more than other drugs; and as a result, only a chosen few at Central State receive it.
That could soon change. Municipal Court Judge Steven Elchholtz ordered hospital officials last month to provide B.W. with the costly drug within 60 days. At a hearing today before Eichholtz, attorneys for the hospital are expected to argue that the judge does not have the right to order the costly medicine.
B.W. is identified only by his initials because records for mental patients are confidential.
It's the first time in Indiana that a judge has ordered officials at a state hospital to provide Clozaril, a drug that has worked wonders on scores of mental patients for whom other treatment has failed.
Advocates for the mentally ill, such as Dee Janik of Protection and Advocacy Services of Indiana, applaud Elchholtz's ruling. For them, this is a right-to-treatment issue --- mental patients are entitled to the best possible care.
B.W. is just one of hundreds of patients in state mental hospitals who might benefit from Clozaril, which has fewer side effects than other medications and offers dramatic improvements from symptoms, Janik said.
Officials from the Indiana Family and Social Services Administration say Eichholtz was playing doctor and overstepped his authority when he ordered the Clozaril for B.W.
Furthermore, the state cannot afford the cost of the drug which is $400 a month, compared with $100 a month for other medications, officials say.
They are planning to appeal and are asking Eichholtz to delay implementing the order. A hearing on that motion is set for this afternoon in Municipal Court 3. The case began as a routine review by Eichholtz of the order to commit B.W. to the state hospital. B.W. through his attorney, James Frank, was asking to be released from the hospital. and the judge convened a hearing to consider the request.
At the hearing, Dr. Steven Conant. B.W.'s psychiatrist, testified that his patient's symptoms were serious enough that he still needs to be hospitalized. The doctor said B.W. can't function independently.
Schizophrenia is a disorder In which patients have distorted thoughts and delusions.
After describing the treatments B.W. has received, Conant said B.W. would be a good candidate for Clozaril. it could reduce his symptoms enough so he could move to a group home. It hasn't been prescribed because of the cost. Conant said. adding. "We don't have the funds to prescribe this for a number of clients for whom we feel it is appropriate."
Up to 75 patIents are good candidates for Clozaril. he said. About 24 currently receive It. hospital officials say.
Conant suggested It could be less expensive for the state to spend the money on Clozaril if It would mean allowing patients to live outside the hospital.
Eichholtz. after ruling that B.W. still needs to be hospitalized, ordered the state to place him on Clozaril within 60 days.
Kathy Gregory, an attorney for the Division of Mental Health, said Eichholtz cannot order a specific treatment as he did In B.W.'s case. Once the judge orders a patient's commitment, mental health officials then determine where and how the patient should receive treatment, she explained.
Said Rachel McGeever, counsel for the family and social services administration: "We wouldn't argue that in the best of all worlds, we would want to provide Clozaril to all who need it." However, the agency must work within its budget and for now, Clozaril is too expensive to be widely distributed. McGeever said. Those budget limits are determined by the legislature and the governor's office.
Barry Irons, director of community services at Central State, said the hospital's medical director and a team of doctors review patient records to determine who will be placed on Clozaril. So patients who don't receive Clozarii are on other drugs like Haldol. one of the most commonly prescribed medications for schizophrenics. Haldol costs about $100 a month, Irons said.That drug has side effects that Include dryness of the mouth. restlessness, drowsiness and severe muscle cramping. Irons said. And it doesn't work on many patients.
Clozaril doesn't have those side effects because it works on a section of the brain that governs emotions and instincts, said Dr. Michael Kane, a consultant to the Division of Mental Health. All of the other drugs. including Haldol. work on the part of the brain governing motor functions. In about 1 percent of all patients, Clozaril causes agranulocytosis - a lowering of the white cell count that leaves the patient susceptible to infection and death. Kane said. So, the manufacturer of Clozaril, Sandoz Pharmaceuticals Corp. of Fairfield, N.J., requires weekly blood tests to monitor the white cell count. That's part of the reason the drug is so expensive.
Now, if Eichholtz's ruling is upheld on appeal, the state could be compelled to find the money to provide patients at the state's mental hospitals with Clozaril. Said Kane: "You're talking about hundreds of patients who could arguably benefit from this medication. It could reduce their symptoms, improve their quality of life."
Click on the article to enlarge.
Go to the lower right corner of the article and right click to enlarge more or print.


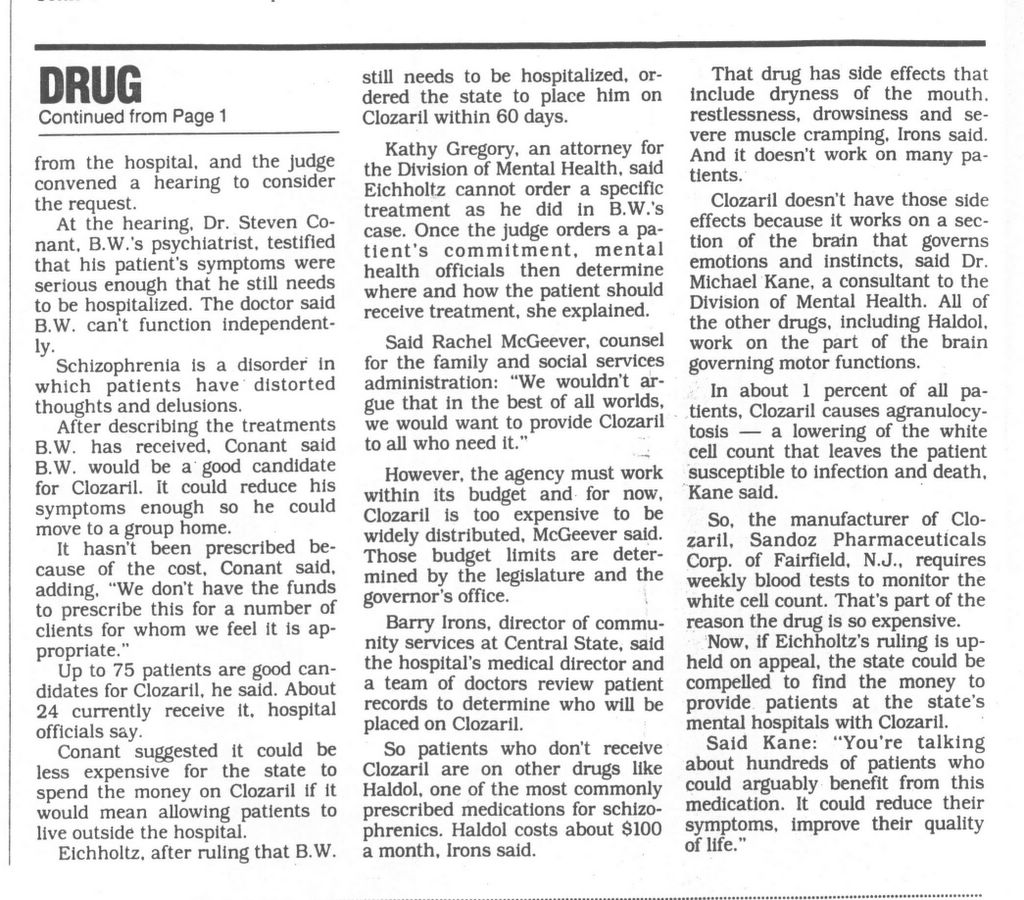
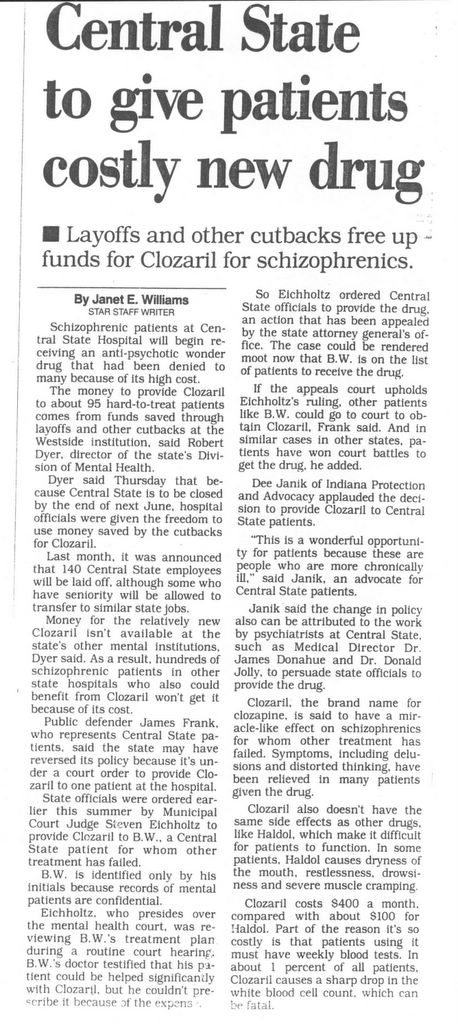
Drug was ordered for schizophrenia, but agency contends it is too costly.
By Janet E. Williams
STAR STAFF WRITER
The Indianapolis Star
B.W.s best hope for overcoming the crippling symptoms of schizophrenia and living outside Central State Hospital is a relatively new drug called Clozaril.
So far, the price tag has kept the anti-psychotic drug beyond his reach. Clozaril costs several times more than other drugs; and as a result, only a chosen few at Central State receive it.
That could soon change. Municipal Court Judge Steven Elchholtz ordered hospital officials last month to provide B.W. with the costly drug within 60 days. At a hearing today before Eichholtz, attorneys for the hospital are expected to argue that the judge does not have the right to order the costly medicine.
B.W. is identified only by his initials because records for mental patients are confidential.
It's the first time in Indiana that a judge has ordered officials at a state hospital to provide Clozaril, a drug that has worked wonders on scores of mental patients for whom other treatment has failed.
Advocates for the mentally ill, such as Dee Janik of Protection and Advocacy Services of Indiana, applaud Elchholtz's ruling. For them, this is a right-to-treatment issue --- mental patients are entitled to the best possible care.
B.W. is just one of hundreds of patients in state mental hospitals who might benefit from Clozaril, which has fewer side effects than other medications and offers dramatic improvements from symptoms, Janik said.
Officials from the Indiana Family and Social Services Administration say Eichholtz was playing doctor and overstepped his authority when he ordered the Clozaril for B.W.
Furthermore, the state cannot afford the cost of the drug which is $400 a month, compared with $100 a month for other medications, officials say.
They are planning to appeal and are asking Eichholtz to delay implementing the order. A hearing on that motion is set for this afternoon in Municipal Court 3. The case began as a routine review by Eichholtz of the order to commit B.W. to the state hospital. B.W. through his attorney, James Frank, was asking to be released from the hospital. and the judge convened a hearing to consider the request.
At the hearing, Dr. Steven Conant. B.W.'s psychiatrist, testified that his patient's symptoms were serious enough that he still needs to be hospitalized. The doctor said B.W. can't function independently.
Schizophrenia is a disorder In which patients have distorted thoughts and delusions.
After describing the treatments B.W. has received, Conant said B.W. would be a good candidate for Clozaril. it could reduce his symptoms enough so he could move to a group home. It hasn't been prescribed because of the cost. Conant said. adding. "We don't have the funds to prescribe this for a number of clients for whom we feel it is appropriate."
Up to 75 patIents are good candidates for Clozaril. he said. About 24 currently receive It. hospital officials say.
Conant suggested It could be less expensive for the state to spend the money on Clozaril if It would mean allowing patients to live outside the hospital.
Eichholtz. after ruling that B.W. still needs to be hospitalized, ordered the state to place him on Clozaril within 60 days.
Kathy Gregory, an attorney for the Division of Mental Health, said Eichholtz cannot order a specific treatment as he did In B.W.'s case. Once the judge orders a patient's commitment, mental health officials then determine where and how the patient should receive treatment, she explained.
Said Rachel McGeever, counsel for the family and social services administration: "We wouldn't argue that in the best of all worlds, we would want to provide Clozaril to all who need it." However, the agency must work within its budget and for now, Clozaril is too expensive to be widely distributed. McGeever said. Those budget limits are determined by the legislature and the governor's office.
Barry Irons, director of community services at Central State, said the hospital's medical director and a team of doctors review patient records to determine who will be placed on Clozaril. So patients who don't receive Clozarii are on other drugs like Haldol. one of the most commonly prescribed medications for schizophrenics. Haldol costs about $100 a month, Irons said.That drug has side effects that Include dryness of the mouth. restlessness, drowsiness and severe muscle cramping. Irons said. And it doesn't work on many patients.
Clozaril doesn't have those side effects because it works on a section of the brain that governs emotions and instincts, said Dr. Michael Kane, a consultant to the Division of Mental Health. All of the other drugs. including Haldol. work on the part of the brain governing motor functions. In about 1 percent of all patients, Clozaril causes agranulocytosis - a lowering of the white cell count that leaves the patient susceptible to infection and death. Kane said. So, the manufacturer of Clozaril, Sandoz Pharmaceuticals Corp. of Fairfield, N.J., requires weekly blood tests to monitor the white cell count. That's part of the reason the drug is so expensive.
Now, if Eichholtz's ruling is upheld on appeal, the state could be compelled to find the money to provide patients at the state's mental hospitals with Clozaril. Said Kane: "You're talking about hundreds of patients who could arguably benefit from this medication. It could reduce their symptoms, improve their quality of life."
Click on the article to enlarge.
Go to the lower right corner of the article and right click to enlarge more or print.
Saturday, January 14, 2006
TAC Newsletter
ENEWS - TREATMENT ADVOCACY CENTER
TREATMENT ADVOCACY CENTER
Visit our web site www.psychlaws.org
January 13, 2006
******************************
1. LAURA'S PARENTS BECOME ADVOCATES FOR CHANGE - Grass Valley Union, January 10,
2006
2. CELEBRATING A SISTER'S MEMORY, ON TAPE - National Public Radio, January 6,
2006
3. CRAZY FOR YOU - MENTAL CASES PACK INTO QUEENS VILLAGE - The New York Post,
January 3, 2006
4. SUICIDE ISN'T SELFISH, BUT SYMPTOM OF ILLNESS - Indianapolis Star, January 3,
2006
5. FALLING THROUGH THE CRACKS - Los Angeles Times, December 24, 200
******************************
1. GRASS VALLEY UNION (CA), January 10, 2006
[Editor’s Note: Great champions of people lost to illnesses like schizophrenia
or bipolar disorder are almost always forged by personal experience. Within the
mental health field impassioned advocates tend to arise from those affected by a
severe mental illness or those who have seen, and lived, the struggles of an
afflicted loved one. In rare instances, however, the fire for treatment comes
all at once from a cataclysmic encounter with the most tragic possible results
of an untreated severe psychiatric disorder.
For Amanda and Nick Wilcox, their zeal for treatment is fueled by the loss of
their daughter, Laura, to the unmedicated paranoid schizophrenia of another.]
LAURA'S PARENTS BECOME ADVOCATES FOR CHANGE
By Dave Moller, Senior staff writer
Five years after their first born was fatally shot on Jan. 10, 2001, Amanda and
Nick Wilcox are still coming to grips with the violent act that took their
daughter and the damage it has done to their family.
“The only justice I could have was Laura back, and I can’t have that,” Amanda
said.
Laura Wilcox, a 19-year-old who was running for student body president at
Haverford College in Pennsylvania, was home visiting on Christmas break that
day. Having served as a summer intern at Nevada County’s Behavioral Health
Department, she was filling in for a sick employee when Scott Thorpe walked
through the front door and started shooting.
Four of his shots found Laura.
“My life felt like it was stripped of meaning because I was a mother,” said
Amanda Wilcox, whose only daughter was the first victim in a shooting spree that
left three dead, three seriously wounded and an entire community on edge.
“I had to focus on other things.”
At the top of that list were her two sons, though Amanda said losing her
daughter sometimes left her afraid to love the boys for fear of losing them,
too.
“Caleb is older than his sister; she was 19,” Amanda said. “There are milestones
like that which put a lump in your throat … I still have days where I don’t stop
crying. (18-year-old) Nathan feels like he was robbed of part of his childhood.”
The families of each of the victims of Jan. 10, 2001 — the day that mental
health patient Scott Thorpe changed the course of their lives — have done their
best to focus on the future. For Amanda and Nick, that has meant being advocates
for change.
“It’s a thin scab; it doesn’t heal easily,” said Nick of losing his daughter.
“It’s been hard, it’s been very hard … We’re good in public, but there are tough
times and tough days.”
While there have been plenty of hard days, healing has also come to the family
in the form of their advocacy against gun violence and the death penalty.
Although they feel Scott Thorpe is rightly incarcerated for life, the Wilcoxes
don’t condone capital punishment.
“We see the death penalty as institutional rage and retribution,” Nick said.
“But our underlying theme is nonviolence.
“The issue picked us. Two years before Laura’s murder, she did a paper on (gun
violence) when she was a junior at (Nevada Union High School).”
“I had always been disturbed by firearm violence anyway,” Amanda said. “We grew
up as Quakers, and one of the basic tenants was nonviolence. Because of our
background, we naturally leaned on that.”
Their advocacy work was kicked into high gear just three weeks after the tragic
shootings, when a gun show was held at the Nevada County Fairgrounds. The
Wilcoxes protested the event as being a possible purveyor to gun violence.
“It was a slap in the face, knowing that Scott Thorpe had been an attendee (of
past shows),” Nick said.
“It was so offensive after what had happened,” Amanda added.
At the show, Nick said, a man approached him to say that had his daughter had a
gun the day she was killed, she would still be alive. Incredulous, Nick took the
comment in a silent, steeled resolve.
The promoter and vendor of the gun show were later arrested for selling illegal
firearms to State Department of Justice agents and were convicted on a
misdemeanor firearms charge. One such gun show followed soon after, but none
have been held locally since, the couple said.
“It made our point,” Amanda said. “We made it too uncomfortable for them and
Nevada County. The promoters did it to themselves.”
Amanda said that the gun-show incident and some law-abiding gun owners did,
however, teach her some new respect for gun owners.
“I’ve learned that my neighbor can have a gun,” she said. “Just because I don’t
like it doesn’t mean they shouldn’t have one.”
Prior to the shooting, Amanda had donated money to the Brady gun control
campaign and the Million Moms March in May of 2000. Now the Wilcoxes find
themselves advocating for much more and with much louder voices.
“We’re effective because of what happened and because we’re not paid,” Nick
said. “We’ve discovered that every legislative door is unlocked.”
One door the couple have walked through belonged to former Assemblywoman Helen
Thompson of Davis. Thompson had put a bill before the legislature in 2001 that
would allow involuntary treatment of mental illness patients if they were a
threat to themselves, or to others, or if they refused treatment after a mental
illness diagnosis.
That bill failed to garner enough support to pass, but it was resurrected into
what is now known as “Laura’s Law” and was passed in 2002. The bill, however,
lacked funding and had conflicting language that could make it difficult to
implement.
The Wilcoxes understand that the provision allowing mental health patients to be
detained involuntarily is highly controversial. Involuntary institutionalization
is what led then Gov. Ronald Reagan to revamp the mental health system in the
1960s.
“But the great promise was never fulfilled to give care in community settings;
it never happened,” Nick said. “There is a strong tendency to deny involuntary
commitment due to cost. But we learned during the trial that Thorpe was the most
mentally ill person the psychiatrists had ever interviewed.”
They also learned that Thorpe had a cache of unregistered weapons, was stalking
a woman at the county’s Behavioral Health Department, and had stopped taking his
medication at the time of the shootings.
It is with no small irony that they learned that soon after Thorpe was put in a
state mental institution for life, he was taking his medication again and doing
much better because of it.
The Laura’s Law experience eventually led the Wilcoxes to the 2004 ballot
initiative Prop. 63, the Mental Health Services Act, which will be used for new
measures for patients across the state. How Laura’s Law will come into effect
with the Prop. 63 funds is still unknown, but the county agreed in its
settlement of a lawsuit with the Wilcoxes to implement it when new funding
becomes available.
“We saw Prop. 63 as something to make a lasting difference, so we donated
$15,000 (to the cause from the $60,000 they were awarded in the settlement.),”
Nick said.
“We’re not experts on mental illness,” Amanda said, “but we helped raise
awareness.”
They are now focused on stopping the use of the death penalty in America and
work closely with a group known as Murder Victims Families for Reconciliation.
This spring, they will testify for a bill asking the state Legislature to
suspend the death penalty until a full examination of its use is completed.
“Whether you’re for or against (the death penalty), it’s unconscionable to
execute innocent victims,” Nick said. “To apply it along social and racial lines
is wrong, even if you support it.”
Part of that belief was bolstered when the Wilcoxes realized that Thorpe did not
target their daughter. They understand that his illness led to Laura’s death and
the eventual apology from the county for not handling it correctly. They also
understand that lawyers may have precluded any official apology; but it still
hurts.
“Victims often just want to hear ‘I’m sorry,’” Amanda said.
“It took a lawsuit and three years to get it,” Nick said. “I still have a lot of
residual anger over how we were treated by Nevada County.”
At the same time, Amanda said, they are focused on the future.
“Scott Thorpe does not have a hold on us.”
******************************
2. NATIONAL PUBLIC RADIO, January 6, 2006
[Editor’s Note: Perhaps the prototype for people who turn grief into the
salvation of others is the Webdale family. Seven years ago, Kendra Webdale was
killed by a man with untreated schizophrenia. That tragic story is well known,
as it was the final straw in getting New York to finally pass an assisted
outpatient treatment law, aptly named “Kendra’s Law.”
This week, NPR presented stirring and saddening memories of Kendra’s sister,
Kim, who strongly endeavored for the law that brought life-stabilizing treatment
to thousands in New York. The interview of Kim Webdale is available at:
http://tacenews.c.topica.com/maaeoAMabnwiqbfGwZEb/ ]
CELEBRATING A SISTER'S MEMORY, ON TAPE
Seven years ago, a young woman named Kendra Webdale was killed when a mentally
ill man pushed her in front of an oncoming New York City subway train. She died
on Jan. 3, 1999.
The case is still in the news, still in the courts, and still very much on the
minds of family members.
Webdale's sister, Kim Emerson, visited one of the Story Corps recording booths
with a friend to recall her sister -- and a cherished reminder of her life.
The Webdale case led to the creation of a new law in New York State -- called
Kendra's Law -- meant to ensure that mentally ill people take the medication
they need.
******************************
3. THE NEW YORK POST, January 3, 2006
[Editor’s Note: The subject of every story that we are interviewed for begs for
responses on the need for earlier interventions, assisted outpatient treatment,
or more hospital beds. Some call for us to present more general themes, as Mary
Zdanowicz offers below by reinforcing the understanding that severe mental
illness is treatable.]
CRAZY FOR YOU - MENTAL CASES PACK INTO QUEENS VILLAGE
By Bill Sanderson and Mark Bulliet
Queens Village has more state-funded housing for the mentally ill than anyplace
else in the city, a Post investigation reveals.
Other neighborhoods with high populations of mentally ill include the Times
Square area, College Point, Queens, the central Rockaways in Queens, and Co-op
City in The Bronx, an analysis of data from the state Office of Mental Health
shows.
But Queens Village - in the shadow of the Creedmoor psychiatric hospital - has
20 state-supported community beds for mentally ill people per every 1,000
residents, 2 1/2 more than Times Square's eight beds per 1,000. Residents and
business owners in Queens Village say they accept the sometimes odd behavior of
their mentally ill neighbors.
"One time, I was cutting a guy's hair, and boom, in the middle of the haircut,
he rips off the cape and leaves," said Ruben Borukhof, a barber on Hillside
Avenue.
"The next morning, he was waiting for me. He said, 'I'm sorry, I didn't take my
medication, and I went off.' "
The unfinished haircut had left the man's hair "lopsided and crazy," Borukhof
recounted. "I said, 'Are we going to finish the haircut, or are you going to
walk around like that?' "
Some mentally ill people need a few minutes longer than other people to phone in
their orders at Szechuan Kitchen, said Susan Zheng, one of the restaurant's
owners. But it's not a problem. "Mostly, they are good, quiet people," Zheng
said.
Over the last few decades, as state hospitals have shrunk, more mentally ill
people moved to houses and apartments. The change has challenged state
government to improve community services for the mentally ill, who studies show
can be violent if they are not being properly treated.
Despite some problems - such as the case of a mentally ill man accused of
savagely stabbing an infant in Washington Heights last September - advocates say
New York has generally done a good job providing community services.
"The public understands that when people are in treatment for mental illness,
they generally do very well," said Mary Zdanowicz, executive director of the
Treatment Advocacy Center, a Washington-based group.
Zdanowicz praised a state law passed after the 1999 attack on Kendra Webdale,
who was killed by a mentally ill man. Kendra's Law requires courts to order
treatment for mentally ill people who don't want it.
******************************
4. INDIANAPOLIS STAR, January 3, 2006
[Editor’s Note: Suicide is a selfish act? Maybe it can be taken that way from
examining its consequences but not, more often than not, after appreciating its
cause.]
Letter to the Editor
SUICIDE ISN'T SELFISH, BUT SYMPTOM OF ILLNESS
Pierre Atlas writes effectively about the terrible tragedy related to the
suicides of youth ("Prominent suicide raises awareness of youth at risk," Dec.
29).
I take special exception to one paragraph in which he describes suicide as an
ultimately selfish act against oneself, friends and family. Suicide is a tragic
symptom of several illnesses such as depression, panic disorder, bipolar
disorder (manic-depressive disorder), schizophrenia and others. Most people with
these illnesses do not take their own lives, but the incidence is significantly
higher than in the general population.
These illnesses are as real as heart disease, diabetes and cancer. Their
symptoms are as physical as headache, chest pain, bone pain and unbearable
nausea. Sometimes the effects of these illnesses on the brain create a different
reality that we are ill prepared to understand. In our sorrow, frustration and
confusion we look for someone to blame. Death from the consequences of illness,
including suicide, is not attributable to anyone's selfishness. Let us join in
community to support each other in solving the problem rather than in assigning
blame.
Joan Esterline Lafuze, Ph.D.
Indianapolis
******************************
5. LOS ANGELES TIMES, December 24, 2005
[Editor’s Note: All those looking for why so many advocates strive for coherent
treatment systems and rational treatment laws, need look no farther than the
life of Marina Lynn Brandt.]
FALLING THROUGH THE CRACKS
Marina Brandt Grew Up In Westchester And Went To UCLA.
Her Descent Into Mental Illness Ended In Death On L.A.'S Skid Row.
By Cara Mia DiMassa, Times Staff Writer
On a sunny May afternoon last year, Marina Lynn Brandt hobbled up to the
cinder-block entrance of the Union Rescue Mission in downtown Los Angeles' skid
row, asking for a bed.
She was thin and pale, her breathing heavy. Her only form of identification was
a plastic hospital band on her right wrist.
Brandt told workers behind the glass contact window that she had been brought to
the mission's San Julian Street entrance by a hospital. One worker, Mary
Witherspoon, said she thought Brandt looked too ill to have been discharged. An
intake clerk began processing her.
Less than an hour after she arrived, Brandt, 45, collapsed on the floor near the
front door. Paramedics tried to revive her, but she was pronounced dead that
evening. The coroner later determined she had died of pneumonia.
"It was kind of devastating," Witherspoon said. "I never had anybody that died
like that. You know so little about them."
Although local hospitals have denied dumping ill patients on skid row, several
have acknowledged routinely transporting medically stable patients there if they
have nowhere else to go. They have defended the practice, saying the area has
the city's greatest concentration of social service agencies.
But as Brandt's story makes clear, some of the patients taken to skid row need
more than social services.
The death made little news at the time, because it was a sadly routine
occurrence on skid row. Like many who call the downtown streets home, Brandt was
mentally ill, with a long history of drug use and the severe health problems
that often accompany it. She had logged years on the streets of Southern
California and been in and out of health facilities across the region.
But a closer look at Brandt's story reveals how a patchwork system of mental
health care and medical services for the indigent often fails some of society's
most desperate, virtually ensuring deaths like hers.
Traditional clinics and hospitals frequently are not equipped to deal with
mental illness. Mental hospitals don't necessarily have facilities to handle
acute physical illness. At the end of her life, Brandt needed both.
"The health system does not work very well for such people," said Marvin
Southard, director of the county Department of Mental Health.
Marina Lynn Brandt grew up in a spacious ranch-style home in Westchester, with a
badminton court and a pool in the backyard, the fourth of five children born to
an aerospace engineer and his wife.
Brandt's father, Ralph, could be loving and generous, said Laura Brandt, the
youngest of the Brandt children. But he also suffered from bipolar illness, and
his behavior could quickly turn frightening.
Sometimes, he set up a lawn chair in a busy intersection near their house,
plunked down on it and opened a beer. Cars would have to swerve to avoid him —
and the police would eventually take him home.
"When he was stabilized, on his meds, it was great," Laura said. "When the
medication wasn't working or it was time to get a dose adjustment, wow. It could
be pretty scary."
Marina earned A's in high school and went to UCLA to study architectural
drafting. But early in her freshman year, she began hearing voices while on
campus. To her family, she seemed forgetful, distracted. They wrote off what
they considered inconsiderate behavior as teenage moodiness.
Soon, though, they realized the problem was more severe. Marina tried to commit
suicide by swallowing pills prescribed for her father. She wandered off for
longer and longer periods.
On one occasion, a family-organized search party found her in downtown Los
Angeles after a long absence. Her hair was matted. She was beaten and bruised.
Her fingers had been burned.
Brandt dropped out of UCLA after the winter quarter of her freshman year. She
was eventually diagnosed with schizophrenia, a chronic and disabling mental
illness.
Downward Spiral
As the disease took hold, Brandt's behavior grew more and more bizarre. She
giggled in public, flirted with strangers who often had no idea of the depths of
her illness. She was easy prey for sexual abuse.
She also became violent, lashing out at those around her.
Laura, who was 10 years younger than her sister, said Brandt would often get a
crazed look in her eyes as the mania set in: "Her eyes would be dilated, glazed
over. The adrenaline was pumping. She looked like a caged animal."
Brandt got that look once at a family gathering just before she tried to choke
her mother. It took three people to pin her down until authorities could arrive
to take her in for psychiatric care.
She got that look again one evening, and her mother and sister had to flee the
house to escape her rage. They returned to find the home ablaze with lights, the
stereo blasting.
"I pretty much tiptoed" in, Laura remembered. "But she saw me — she was still
awake, and she came after me with two kitchen knives."
In the first few years of Brandt's illness, she racked up a string of
hospitalizations, for both psychiatric and physical ills, as well as multiple
arrests. By the end of 1983, it was clear she could no longer care for herself.
She was put under a conservatorship, with the Los Angeles County public
guardian's office acting as conservator.
In a 1984 court filing, the deputy public guardian assigned to her case, Vaishie
Lazaire, described the difficulty of overseeing Brandt's care.
"She wanders the streets ingesting any and all drugs and alcohol offered her and
is unable to obtain adequate food or shelter," Lazaire wrote. "She has been
repeatedly raped and beaten while wandering on the streets. She often refuses to
eat for long periods of time because 'voices tell her she is fat.' … Marina Lynn
remains too psychotic to make rational decisions for herself."
A Home in Pomona
In 1984, after years of struggling with his own demons, Ralph Brandt drowned
himself in the family swimming pool.
In the wake of his death, the family established a special trust to help take
care of Marina financially.
Her mother had pinched pennies for years to buy a string of houses, apartment
buildings and land around Southern California. The sale of one of those
properties, a house on Grimsby Avenue in Westchester, brought $121,000, which
was put into a trust for Marina administered by the public guardian's office.
That money, combined with a monthly disability stipend and occasional Christmas
gifts of a few hundred dollars from Brandt's mother, paid for nearly a decade of
Brandt's care, mostly at what was by then her full-time home, Landmark Medical
Center in Pomona.
In retrospect, sister Laura said, the period at Landmark was the most stable in
Brandt's adult life.
But her stay was not entirely problem-free.
In January 1985, Dr. William E. Sigurdson, Brandt's doctor, wrote that she was
"confused and delusional. She frequently gets into fights, believing that people
are talking about her. She … could become violent, with resultant injury to self
or others."
A few years later, Brandt disappeared from the facility and wound up in San Luis
Obispo; she was returned by Greyhound bus.
In January 1993, she was arrested in Glendale for public intoxication.
In 1995, the money from her father's estate ran out. Soon after, she left
Landmark. Laura Brandt said her departure baffled family members, but they
suspected that her running out of money was a factor.
Rosemary Campos Kilby, Landmark's administrator, said she couldn't comment on
the specifics of Brandt's stay. But she strongly denied any implication that a
patient would have been turned out for financial reasons.
She said that "most of the people who live here are on county funding…. If her
money had run out, it would not have meant a difference to the facility."
Regardless, life after her trust fund dried up proved far less stable for
Brandt.
A String of Hospitals
After Landmark, the shuffle began.
Court records show that Brandt bounced around Southern California for the next
nine years. She was in and out of mental hospitals, treatment facilities and
regular hospitals across the Southland, including stops in Rancho Cucamonga,
Whittier, San Gabriel, Venice and El Monte, among other places.
Family members tried to keep up with her movements but found it difficult, said
Laura Brandt: "There were so many facilities, just too many to remember.
"Sometimes, the best night's sleep I had was when she was in a locked, good
facility," she said.
The public guardian's office recorded 70 addresses for Brandt in the time she
was in its care.
Sometimes, the move from one facility to another came after Brandt got in
trouble for drug or alcohol use.
Other times, she just walked out and disappeared for days or weeks at a time,
unable or unwilling to return.
"That was a pretty common thing, where she would get lost from her own
facility," Laura said. "They moved her around so much, it would be easy for her
to forget."
In 2003, Brandt walked out of a Los Angeles facility, saying she preferred
living on the streets. Almost three weeks later, she was admitted to a
psychiatric hospital in Alhambra.
Later that year, she told workers at a Pomona board-and-care home that she was
going out to a local 99 Cent store; the next day, they reported her to police as
missing. She resurfaced a few days later at Kaiser Permanente in Hollywood.
As the years ticked by, Brandt's physical health deteriorated. Life on the
streets, between her stays in medical facilities, wore on her. She contracted
HIV. She was diagnosed with breast cancer and in 2001 underwent a mastectomy.
She suffered bouts of anorexia.
Brandt, who records show was 5 feet 5, weighed about 80 pounds in 2003.
The pace of her movement from one facility to another seemed to quicken late
that year, six months before her death. She was admitted to Greater El Monte
Community Hospital the first week of January 2004 to have an abscess in her
chest drained. She told doctors she feared that her earlier cancer was
returning, especially because her twin brother, James, had died of lung cancer
in 1994.
After nine days, Brandt was moved to San Gabriel Valley Medical Center in San
Gabriel, where she underwent psychiatric evaluation and treatment.
From there, she was moved to Brighton Convalescent Center, a long-term care
facility in Pasadena. That stay was interrupted after six weeks, when Brandt
started having seizures. She also was bleeding from her right eye.
At Alhambra Community Hospital, where she was treated, a doctor noted that in
addition to previous ailments, she had multiple infections associated with
methicillin-resistant Staphylococcus aureus (MRSA), an infection prevalent on
the streets and in jails, and commonly seen in AIDS patients. She was severely
anemic. She also had a shortage of all types of blood cells, including those
that fight off infection.
Brandt was returned to the convalescent center four days later. But she was not
a willing patient. She tried to refuse an IV from nurses. She wouldn't wear a
mask to limit other patients' exposure to her infections. She threatened to
leave the facility.
During this particularly difficult period in Brandt's life, the public
guardian's office seemed to take very little role. Her file contains only two
notations in 2004 before her death in May.
Citing privacy concerns, the office refused to comment on the specifics of
Brandt's case. But spokesman Chris Fiero said that dealing with mentally ill
clients can be "extremely difficult."
His office, he says, does "the best that we can to try to arrange appropriate
living arrangements and appropriate care for all of our clients. But sometimes
the needs of the client overwhelm our ability to adequately meet those needs."
Residential facilities can also feel overwhelmed.
Steven Pavlow, the licensed operator of Brighton Convalescent Center, said in an
interview that because Brandt had developed AIDS, his facility had no choice but
to accept her as a patient when she arrived in February 2004. But he has doubts
about whether centers like his are the best place for mentally ill patients.
"Under the federal guidelines, we have no choice," Pavlow said. "And when there
are psychiatric issues, you do the best you can."
After changes in the laws about mental health care in the late 1960s, skilled
nursing facilities like his, he said, "became sort of by default the facility
for almost any kind of illness. We treat them medically, we have psychiatric
consultations, but we have absolutely no rights as a skilled nursing facility to
hold them."
On April 12, 2004, Brandt left Brighton against medical advice.
Mysteries Remain
The final weeks of Brandt's life are murky.
Late in the evening of April 29, she was admitted to the emergency room of Good
Samaritan Hospital, west of downtown Los Angeles. She had a fever and difficulty
breathing. By 2 a.m. she was back on the street.
Jess Beattie, a social worker in the emergency room, said the hospital provided
Brandt with "medical care, food, new clothing and a shower" before discharging
her.
"From my standpoint, the care was appropriate," said Phil Fagan, director of the
emergency room. "She was, on discharge, better than when she came in."
Her whereabouts are unknown between then and 2:45 p.m. May 1, when she arrived
at the Union Rescue Mission.
One intake worker there, Stephanie Davenport, says a man she thought might have
been a taxi driver brought Brandt to the mission. Brandt said she'd been sent by
a hospital and provided a doctor's note, according to a mission log.
Mission officials say they don't know what happened to that note, and the
coroner's office says it was not among her possessions.
At the time of Brandt's death, her sister Laura was trying to locate her. In
mid-May, Laura arrived home one evening to find a letter from the county
coroner. Marina Brandt was dead.
She had died of lobar pneumonia, an ailment often associated with a compromised
immune system. There was so much infection in her right lung that it weighed
almost three times as much as her left. There were no alcohol or illegal drugs
in her system.
Laura said she is appalled to think that a hospital might have abandoned Brandt
at the time when she so clearly needed medical attention.
But the way the system worked, she said, "I am amazed that she lived to the age
of 45."
******************************
Treatment Advocacy Center E-NEWS is a publication of the Treatment Advocacy
Center.
This E-NEWS is provided as a public service by the Treatment Advocacy Center.
There is no fee. If you would also like to receive a free subscription to the
Catalyst, our quarterly hardcopy newsletter, please forward your mailing address
to info@psychlaws.org.
The Center does not accept donations from pharmaceutical companies. Support
from individuals who share our mission, however, is essential to our ability to
effectively help our most vulnerable citizens. The Treatment Advocacy Center is
a 501(c)(3) not-for-profit organization. All contributions are tax-deductible
to the extent allowed by law. Donations to the Treatment Advocacy Center should
be sent to:
Treatment Advocacy Center
200 North Glebe Road, Suite 730
Arlington, VA 22203
703-294-6001 (main no.)
703-294-6010 (fax)
TREATMENT ADVOCACY CENTER
Visit our web site www.psychlaws.org
January 13, 2006
******************************
1. LAURA'S PARENTS BECOME ADVOCATES FOR CHANGE - Grass Valley Union, January 10,
2006
2. CELEBRATING A SISTER'S MEMORY, ON TAPE - National Public Radio, January 6,
2006
3. CRAZY FOR YOU - MENTAL CASES PACK INTO QUEENS VILLAGE - The New York Post,
January 3, 2006
4. SUICIDE ISN'T SELFISH, BUT SYMPTOM OF ILLNESS - Indianapolis Star, January 3,
2006
5. FALLING THROUGH THE CRACKS - Los Angeles Times, December 24, 200
******************************
1. GRASS VALLEY UNION (CA), January 10, 2006
[Editor’s Note: Great champions of people lost to illnesses like schizophrenia
or bipolar disorder are almost always forged by personal experience. Within the
mental health field impassioned advocates tend to arise from those affected by a
severe mental illness or those who have seen, and lived, the struggles of an
afflicted loved one. In rare instances, however, the fire for treatment comes
all at once from a cataclysmic encounter with the most tragic possible results
of an untreated severe psychiatric disorder.
For Amanda and Nick Wilcox, their zeal for treatment is fueled by the loss of
their daughter, Laura, to the unmedicated paranoid schizophrenia of another.]
LAURA'S PARENTS BECOME ADVOCATES FOR CHANGE
By Dave Moller, Senior staff writer
Five years after their first born was fatally shot on Jan. 10, 2001, Amanda and
Nick Wilcox are still coming to grips with the violent act that took their
daughter and the damage it has done to their family.
“The only justice I could have was Laura back, and I can’t have that,” Amanda
said.
Laura Wilcox, a 19-year-old who was running for student body president at
Haverford College in Pennsylvania, was home visiting on Christmas break that
day. Having served as a summer intern at Nevada County’s Behavioral Health
Department, she was filling in for a sick employee when Scott Thorpe walked
through the front door and started shooting.
Four of his shots found Laura.
“My life felt like it was stripped of meaning because I was a mother,” said
Amanda Wilcox, whose only daughter was the first victim in a shooting spree that
left three dead, three seriously wounded and an entire community on edge.
“I had to focus on other things.”
At the top of that list were her two sons, though Amanda said losing her
daughter sometimes left her afraid to love the boys for fear of losing them,
too.
“Caleb is older than his sister; she was 19,” Amanda said. “There are milestones
like that which put a lump in your throat … I still have days where I don’t stop
crying. (18-year-old) Nathan feels like he was robbed of part of his childhood.”
The families of each of the victims of Jan. 10, 2001 — the day that mental
health patient Scott Thorpe changed the course of their lives — have done their
best to focus on the future. For Amanda and Nick, that has meant being advocates
for change.
“It’s a thin scab; it doesn’t heal easily,” said Nick of losing his daughter.
“It’s been hard, it’s been very hard … We’re good in public, but there are tough
times and tough days.”
While there have been plenty of hard days, healing has also come to the family
in the form of their advocacy against gun violence and the death penalty.
Although they feel Scott Thorpe is rightly incarcerated for life, the Wilcoxes
don’t condone capital punishment.
“We see the death penalty as institutional rage and retribution,” Nick said.
“But our underlying theme is nonviolence.
“The issue picked us. Two years before Laura’s murder, she did a paper on (gun
violence) when she was a junior at (Nevada Union High School).”
“I had always been disturbed by firearm violence anyway,” Amanda said. “We grew
up as Quakers, and one of the basic tenants was nonviolence. Because of our
background, we naturally leaned on that.”
Their advocacy work was kicked into high gear just three weeks after the tragic
shootings, when a gun show was held at the Nevada County Fairgrounds. The
Wilcoxes protested the event as being a possible purveyor to gun violence.
“It was a slap in the face, knowing that Scott Thorpe had been an attendee (of
past shows),” Nick said.
“It was so offensive after what had happened,” Amanda added.
At the show, Nick said, a man approached him to say that had his daughter had a
gun the day she was killed, she would still be alive. Incredulous, Nick took the
comment in a silent, steeled resolve.
The promoter and vendor of the gun show were later arrested for selling illegal
firearms to State Department of Justice agents and were convicted on a
misdemeanor firearms charge. One such gun show followed soon after, but none
have been held locally since, the couple said.
“It made our point,” Amanda said. “We made it too uncomfortable for them and
Nevada County. The promoters did it to themselves.”
Amanda said that the gun-show incident and some law-abiding gun owners did,
however, teach her some new respect for gun owners.
“I’ve learned that my neighbor can have a gun,” she said. “Just because I don’t
like it doesn’t mean they shouldn’t have one.”
Prior to the shooting, Amanda had donated money to the Brady gun control
campaign and the Million Moms March in May of 2000. Now the Wilcoxes find
themselves advocating for much more and with much louder voices.
“We’re effective because of what happened and because we’re not paid,” Nick
said. “We’ve discovered that every legislative door is unlocked.”
One door the couple have walked through belonged to former Assemblywoman Helen
Thompson of Davis. Thompson had put a bill before the legislature in 2001 that
would allow involuntary treatment of mental illness patients if they were a
threat to themselves, or to others, or if they refused treatment after a mental
illness diagnosis.
That bill failed to garner enough support to pass, but it was resurrected into
what is now known as “Laura’s Law” and was passed in 2002. The bill, however,
lacked funding and had conflicting language that could make it difficult to
implement.
The Wilcoxes understand that the provision allowing mental health patients to be
detained involuntarily is highly controversial. Involuntary institutionalization
is what led then Gov. Ronald Reagan to revamp the mental health system in the
1960s.
“But the great promise was never fulfilled to give care in community settings;
it never happened,” Nick said. “There is a strong tendency to deny involuntary
commitment due to cost. But we learned during the trial that Thorpe was the most
mentally ill person the psychiatrists had ever interviewed.”
They also learned that Thorpe had a cache of unregistered weapons, was stalking
a woman at the county’s Behavioral Health Department, and had stopped taking his
medication at the time of the shootings.
It is with no small irony that they learned that soon after Thorpe was put in a
state mental institution for life, he was taking his medication again and doing
much better because of it.
The Laura’s Law experience eventually led the Wilcoxes to the 2004 ballot
initiative Prop. 63, the Mental Health Services Act, which will be used for new
measures for patients across the state. How Laura’s Law will come into effect
with the Prop. 63 funds is still unknown, but the county agreed in its
settlement of a lawsuit with the Wilcoxes to implement it when new funding
becomes available.
“We saw Prop. 63 as something to make a lasting difference, so we donated
$15,000 (to the cause from the $60,000 they were awarded in the settlement.),”
Nick said.
“We’re not experts on mental illness,” Amanda said, “but we helped raise
awareness.”
They are now focused on stopping the use of the death penalty in America and
work closely with a group known as Murder Victims Families for Reconciliation.
This spring, they will testify for a bill asking the state Legislature to
suspend the death penalty until a full examination of its use is completed.
“Whether you’re for or against (the death penalty), it’s unconscionable to
execute innocent victims,” Nick said. “To apply it along social and racial lines
is wrong, even if you support it.”
Part of that belief was bolstered when the Wilcoxes realized that Thorpe did not
target their daughter. They understand that his illness led to Laura’s death and
the eventual apology from the county for not handling it correctly. They also
understand that lawyers may have precluded any official apology; but it still
hurts.
“Victims often just want to hear ‘I’m sorry,’” Amanda said.
“It took a lawsuit and three years to get it,” Nick said. “I still have a lot of
residual anger over how we were treated by Nevada County.”
At the same time, Amanda said, they are focused on the future.
“Scott Thorpe does not have a hold on us.”
******************************
2. NATIONAL PUBLIC RADIO, January 6, 2006
[Editor’s Note: Perhaps the prototype for people who turn grief into the
salvation of others is the Webdale family. Seven years ago, Kendra Webdale was
killed by a man with untreated schizophrenia. That tragic story is well known,
as it was the final straw in getting New York to finally pass an assisted
outpatient treatment law, aptly named “Kendra’s Law.”
This week, NPR presented stirring and saddening memories of Kendra’s sister,
Kim, who strongly endeavored for the law that brought life-stabilizing treatment
to thousands in New York. The interview of Kim Webdale is available at:
http://tacenews.c.topica.com/maaeoAMabnwiqbfGwZEb/ ]
CELEBRATING A SISTER'S MEMORY, ON TAPE
Seven years ago, a young woman named Kendra Webdale was killed when a mentally
ill man pushed her in front of an oncoming New York City subway train. She died
on Jan. 3, 1999.
The case is still in the news, still in the courts, and still very much on the
minds of family members.
Webdale's sister, Kim Emerson, visited one of the Story Corps recording booths
with a friend to recall her sister -- and a cherished reminder of her life.
The Webdale case led to the creation of a new law in New York State -- called
Kendra's Law -- meant to ensure that mentally ill people take the medication
they need.
******************************
3. THE NEW YORK POST, January 3, 2006
[Editor’s Note: The subject of every story that we are interviewed for begs for
responses on the need for earlier interventions, assisted outpatient treatment,
or more hospital beds. Some call for us to present more general themes, as Mary
Zdanowicz offers below by reinforcing the understanding that severe mental
illness is treatable.]
CRAZY FOR YOU - MENTAL CASES PACK INTO QUEENS VILLAGE
By Bill Sanderson and Mark Bulliet
Queens Village has more state-funded housing for the mentally ill than anyplace
else in the city, a Post investigation reveals.
Other neighborhoods with high populations of mentally ill include the Times
Square area, College Point, Queens, the central Rockaways in Queens, and Co-op
City in The Bronx, an analysis of data from the state Office of Mental Health
shows.
But Queens Village - in the shadow of the Creedmoor psychiatric hospital - has
20 state-supported community beds for mentally ill people per every 1,000
residents, 2 1/2 more than Times Square's eight beds per 1,000. Residents and
business owners in Queens Village say they accept the sometimes odd behavior of
their mentally ill neighbors.
"One time, I was cutting a guy's hair, and boom, in the middle of the haircut,
he rips off the cape and leaves," said Ruben Borukhof, a barber on Hillside
Avenue.
"The next morning, he was waiting for me. He said, 'I'm sorry, I didn't take my
medication, and I went off.' "
The unfinished haircut had left the man's hair "lopsided and crazy," Borukhof
recounted. "I said, 'Are we going to finish the haircut, or are you going to
walk around like that?' "
Some mentally ill people need a few minutes longer than other people to phone in
their orders at Szechuan Kitchen, said Susan Zheng, one of the restaurant's
owners. But it's not a problem. "Mostly, they are good, quiet people," Zheng
said.
Over the last few decades, as state hospitals have shrunk, more mentally ill
people moved to houses and apartments. The change has challenged state
government to improve community services for the mentally ill, who studies show
can be violent if they are not being properly treated.
Despite some problems - such as the case of a mentally ill man accused of
savagely stabbing an infant in Washington Heights last September - advocates say
New York has generally done a good job providing community services.
"The public understands that when people are in treatment for mental illness,
they generally do very well," said Mary Zdanowicz, executive director of the
Treatment Advocacy Center, a Washington-based group.
Zdanowicz praised a state law passed after the 1999 attack on Kendra Webdale,
who was killed by a mentally ill man. Kendra's Law requires courts to order
treatment for mentally ill people who don't want it.
******************************
4. INDIANAPOLIS STAR, January 3, 2006
[Editor’s Note: Suicide is a selfish act? Maybe it can be taken that way from
examining its consequences but not, more often than not, after appreciating its
cause.]
Letter to the Editor
SUICIDE ISN'T SELFISH, BUT SYMPTOM OF ILLNESS
Pierre Atlas writes effectively about the terrible tragedy related to the
suicides of youth ("Prominent suicide raises awareness of youth at risk," Dec.
29).
I take special exception to one paragraph in which he describes suicide as an
ultimately selfish act against oneself, friends and family. Suicide is a tragic
symptom of several illnesses such as depression, panic disorder, bipolar
disorder (manic-depressive disorder), schizophrenia and others. Most people with
these illnesses do not take their own lives, but the incidence is significantly
higher than in the general population.
These illnesses are as real as heart disease, diabetes and cancer. Their
symptoms are as physical as headache, chest pain, bone pain and unbearable
nausea. Sometimes the effects of these illnesses on the brain create a different
reality that we are ill prepared to understand. In our sorrow, frustration and
confusion we look for someone to blame. Death from the consequences of illness,
including suicide, is not attributable to anyone's selfishness. Let us join in
community to support each other in solving the problem rather than in assigning
blame.
Joan Esterline Lafuze, Ph.D.
Indianapolis
******************************
5. LOS ANGELES TIMES, December 24, 2005
[Editor’s Note: All those looking for why so many advocates strive for coherent
treatment systems and rational treatment laws, need look no farther than the
life of Marina Lynn Brandt.]
FALLING THROUGH THE CRACKS
Marina Brandt Grew Up In Westchester And Went To UCLA.
Her Descent Into Mental Illness Ended In Death On L.A.'S Skid Row.
By Cara Mia DiMassa, Times Staff Writer
On a sunny May afternoon last year, Marina Lynn Brandt hobbled up to the
cinder-block entrance of the Union Rescue Mission in downtown Los Angeles' skid
row, asking for a bed.
She was thin and pale, her breathing heavy. Her only form of identification was
a plastic hospital band on her right wrist.
Brandt told workers behind the glass contact window that she had been brought to
the mission's San Julian Street entrance by a hospital. One worker, Mary
Witherspoon, said she thought Brandt looked too ill to have been discharged. An
intake clerk began processing her.
Less than an hour after she arrived, Brandt, 45, collapsed on the floor near the
front door. Paramedics tried to revive her, but she was pronounced dead that
evening. The coroner later determined she had died of pneumonia.
"It was kind of devastating," Witherspoon said. "I never had anybody that died
like that. You know so little about them."
Although local hospitals have denied dumping ill patients on skid row, several
have acknowledged routinely transporting medically stable patients there if they
have nowhere else to go. They have defended the practice, saying the area has
the city's greatest concentration of social service agencies.
But as Brandt's story makes clear, some of the patients taken to skid row need
more than social services.
The death made little news at the time, because it was a sadly routine
occurrence on skid row. Like many who call the downtown streets home, Brandt was
mentally ill, with a long history of drug use and the severe health problems
that often accompany it. She had logged years on the streets of Southern
California and been in and out of health facilities across the region.
But a closer look at Brandt's story reveals how a patchwork system of mental
health care and medical services for the indigent often fails some of society's
most desperate, virtually ensuring deaths like hers.
Traditional clinics and hospitals frequently are not equipped to deal with
mental illness. Mental hospitals don't necessarily have facilities to handle
acute physical illness. At the end of her life, Brandt needed both.
"The health system does not work very well for such people," said Marvin
Southard, director of the county Department of Mental Health.
Marina Lynn Brandt grew up in a spacious ranch-style home in Westchester, with a
badminton court and a pool in the backyard, the fourth of five children born to
an aerospace engineer and his wife.
Brandt's father, Ralph, could be loving and generous, said Laura Brandt, the
youngest of the Brandt children. But he also suffered from bipolar illness, and
his behavior could quickly turn frightening.
Sometimes, he set up a lawn chair in a busy intersection near their house,
plunked down on it and opened a beer. Cars would have to swerve to avoid him —
and the police would eventually take him home.
"When he was stabilized, on his meds, it was great," Laura said. "When the
medication wasn't working or it was time to get a dose adjustment, wow. It could
be pretty scary."
Marina earned A's in high school and went to UCLA to study architectural
drafting. But early in her freshman year, she began hearing voices while on
campus. To her family, she seemed forgetful, distracted. They wrote off what
they considered inconsiderate behavior as teenage moodiness.
Soon, though, they realized the problem was more severe. Marina tried to commit
suicide by swallowing pills prescribed for her father. She wandered off for
longer and longer periods.
On one occasion, a family-organized search party found her in downtown Los
Angeles after a long absence. Her hair was matted. She was beaten and bruised.
Her fingers had been burned.
Brandt dropped out of UCLA after the winter quarter of her freshman year. She
was eventually diagnosed with schizophrenia, a chronic and disabling mental
illness.
Downward Spiral
As the disease took hold, Brandt's behavior grew more and more bizarre. She
giggled in public, flirted with strangers who often had no idea of the depths of
her illness. She was easy prey for sexual abuse.
She also became violent, lashing out at those around her.
Laura, who was 10 years younger than her sister, said Brandt would often get a
crazed look in her eyes as the mania set in: "Her eyes would be dilated, glazed
over. The adrenaline was pumping. She looked like a caged animal."
Brandt got that look once at a family gathering just before she tried to choke
her mother. It took three people to pin her down until authorities could arrive
to take her in for psychiatric care.
She got that look again one evening, and her mother and sister had to flee the
house to escape her rage. They returned to find the home ablaze with lights, the
stereo blasting.
"I pretty much tiptoed" in, Laura remembered. "But she saw me — she was still
awake, and she came after me with two kitchen knives."
In the first few years of Brandt's illness, she racked up a string of
hospitalizations, for both psychiatric and physical ills, as well as multiple
arrests. By the end of 1983, it was clear she could no longer care for herself.
She was put under a conservatorship, with the Los Angeles County public
guardian's office acting as conservator.
In a 1984 court filing, the deputy public guardian assigned to her case, Vaishie
Lazaire, described the difficulty of overseeing Brandt's care.
"She wanders the streets ingesting any and all drugs and alcohol offered her and
is unable to obtain adequate food or shelter," Lazaire wrote. "She has been
repeatedly raped and beaten while wandering on the streets. She often refuses to
eat for long periods of time because 'voices tell her she is fat.' … Marina Lynn
remains too psychotic to make rational decisions for herself."
A Home in Pomona
In 1984, after years of struggling with his own demons, Ralph Brandt drowned
himself in the family swimming pool.
In the wake of his death, the family established a special trust to help take
care of Marina financially.
Her mother had pinched pennies for years to buy a string of houses, apartment
buildings and land around Southern California. The sale of one of those
properties, a house on Grimsby Avenue in Westchester, brought $121,000, which
was put into a trust for Marina administered by the public guardian's office.
That money, combined with a monthly disability stipend and occasional Christmas
gifts of a few hundred dollars from Brandt's mother, paid for nearly a decade of
Brandt's care, mostly at what was by then her full-time home, Landmark Medical
Center in Pomona.
In retrospect, sister Laura said, the period at Landmark was the most stable in
Brandt's adult life.
But her stay was not entirely problem-free.
In January 1985, Dr. William E. Sigurdson, Brandt's doctor, wrote that she was
"confused and delusional. She frequently gets into fights, believing that people
are talking about her. She … could become violent, with resultant injury to self
or others."
A few years later, Brandt disappeared from the facility and wound up in San Luis
Obispo; she was returned by Greyhound bus.
In January 1993, she was arrested in Glendale for public intoxication.
In 1995, the money from her father's estate ran out. Soon after, she left
Landmark. Laura Brandt said her departure baffled family members, but they
suspected that her running out of money was a factor.
Rosemary Campos Kilby, Landmark's administrator, said she couldn't comment on
the specifics of Brandt's stay. But she strongly denied any implication that a
patient would have been turned out for financial reasons.
She said that "most of the people who live here are on county funding…. If her
money had run out, it would not have meant a difference to the facility."
Regardless, life after her trust fund dried up proved far less stable for
Brandt.
A String of Hospitals
After Landmark, the shuffle began.
Court records show that Brandt bounced around Southern California for the next
nine years. She was in and out of mental hospitals, treatment facilities and
regular hospitals across the Southland, including stops in Rancho Cucamonga,
Whittier, San Gabriel, Venice and El Monte, among other places.
Family members tried to keep up with her movements but found it difficult, said
Laura Brandt: "There were so many facilities, just too many to remember.
"Sometimes, the best night's sleep I had was when she was in a locked, good
facility," she said.
The public guardian's office recorded 70 addresses for Brandt in the time she
was in its care.
Sometimes, the move from one facility to another came after Brandt got in
trouble for drug or alcohol use.
Other times, she just walked out and disappeared for days or weeks at a time,
unable or unwilling to return.
"That was a pretty common thing, where she would get lost from her own
facility," Laura said. "They moved her around so much, it would be easy for her
to forget."
In 2003, Brandt walked out of a Los Angeles facility, saying she preferred
living on the streets. Almost three weeks later, she was admitted to a
psychiatric hospital in Alhambra.
Later that year, she told workers at a Pomona board-and-care home that she was
going out to a local 99 Cent store; the next day, they reported her to police as
missing. She resurfaced a few days later at Kaiser Permanente in Hollywood.
As the years ticked by, Brandt's physical health deteriorated. Life on the
streets, between her stays in medical facilities, wore on her. She contracted
HIV. She was diagnosed with breast cancer and in 2001 underwent a mastectomy.
She suffered bouts of anorexia.
Brandt, who records show was 5 feet 5, weighed about 80 pounds in 2003.
The pace of her movement from one facility to another seemed to quicken late
that year, six months before her death. She was admitted to Greater El Monte
Community Hospital the first week of January 2004 to have an abscess in her
chest drained. She told doctors she feared that her earlier cancer was
returning, especially because her twin brother, James, had died of lung cancer
in 1994.
After nine days, Brandt was moved to San Gabriel Valley Medical Center in San
Gabriel, where she underwent psychiatric evaluation and treatment.
From there, she was moved to Brighton Convalescent Center, a long-term care
facility in Pasadena. That stay was interrupted after six weeks, when Brandt
started having seizures. She also was bleeding from her right eye.
At Alhambra Community Hospital, where she was treated, a doctor noted that in
addition to previous ailments, she had multiple infections associated with
methicillin-resistant Staphylococcus aureus (MRSA), an infection prevalent on
the streets and in jails, and commonly seen in AIDS patients. She was severely
anemic. She also had a shortage of all types of blood cells, including those
that fight off infection.
Brandt was returned to the convalescent center four days later. But she was not
a willing patient. She tried to refuse an IV from nurses. She wouldn't wear a
mask to limit other patients' exposure to her infections. She threatened to
leave the facility.
During this particularly difficult period in Brandt's life, the public
guardian's office seemed to take very little role. Her file contains only two
notations in 2004 before her death in May.
Citing privacy concerns, the office refused to comment on the specifics of
Brandt's case. But spokesman Chris Fiero said that dealing with mentally ill
clients can be "extremely difficult."
His office, he says, does "the best that we can to try to arrange appropriate
living arrangements and appropriate care for all of our clients. But sometimes
the needs of the client overwhelm our ability to adequately meet those needs."
Residential facilities can also feel overwhelmed.
Steven Pavlow, the licensed operator of Brighton Convalescent Center, said in an
interview that because Brandt had developed AIDS, his facility had no choice but
to accept her as a patient when she arrived in February 2004. But he has doubts
about whether centers like his are the best place for mentally ill patients.
"Under the federal guidelines, we have no choice," Pavlow said. "And when there
are psychiatric issues, you do the best you can."
After changes in the laws about mental health care in the late 1960s, skilled
nursing facilities like his, he said, "became sort of by default the facility
for almost any kind of illness. We treat them medically, we have psychiatric
consultations, but we have absolutely no rights as a skilled nursing facility to
hold them."
On April 12, 2004, Brandt left Brighton against medical advice.
Mysteries Remain
The final weeks of Brandt's life are murky.
Late in the evening of April 29, she was admitted to the emergency room of Good
Samaritan Hospital, west of downtown Los Angeles. She had a fever and difficulty
breathing. By 2 a.m. she was back on the street.
Jess Beattie, a social worker in the emergency room, said the hospital provided
Brandt with "medical care, food, new clothing and a shower" before discharging
her.
"From my standpoint, the care was appropriate," said Phil Fagan, director of the
emergency room. "She was, on discharge, better than when she came in."
Her whereabouts are unknown between then and 2:45 p.m. May 1, when she arrived
at the Union Rescue Mission.
One intake worker there, Stephanie Davenport, says a man she thought might have
been a taxi driver brought Brandt to the mission. Brandt said she'd been sent by
a hospital and provided a doctor's note, according to a mission log.
Mission officials say they don't know what happened to that note, and the
coroner's office says it was not among her possessions.
At the time of Brandt's death, her sister Laura was trying to locate her. In
mid-May, Laura arrived home one evening to find a letter from the county
coroner. Marina Brandt was dead.
She had died of lobar pneumonia, an ailment often associated with a compromised
immune system. There was so much infection in her right lung that it weighed
almost three times as much as her left. There were no alcohol or illegal drugs
in her system.
Laura said she is appalled to think that a hospital might have abandoned Brandt
at the time when she so clearly needed medical attention.
But the way the system worked, she said, "I am amazed that she lived to the age
of 45."
******************************
Treatment Advocacy Center E-NEWS is a publication of the Treatment Advocacy
Center.
This E-NEWS is provided as a public service by the Treatment Advocacy Center.
There is no fee. If you would also like to receive a free subscription to the
Catalyst, our quarterly hardcopy newsletter, please forward your mailing address
to info@psychlaws.org.
The Center does not accept donations from pharmaceutical companies. Support
from individuals who share our mission, however, is essential to our ability to
effectively help our most vulnerable citizens. The Treatment Advocacy Center is
a 501(c)(3) not-for-profit organization. All contributions are tax-deductible
to the extent allowed by law. Donations to the Treatment Advocacy Center should
be sent to:
Treatment Advocacy Center
200 North Glebe Road, Suite 730
Arlington, VA 22203
703-294-6001 (main no.)
703-294-6010 (fax)
![]()