Sunday, January 30, 2005
Art of the Mentally Ill
Saturday, January 29, 2005
The Man Who Held Mental Health Law Hostage

Quote from the Indianapolis Star, 1/29/05:
"Anthony G. "Tony" Kiritsis, who made national headlines when he wired a sawed-off shotgun around the neck of an Indianapolis mortgage company executive in 1977 and paraded him through Downtown streets, was found dead in his home Friday.
The incident would forever change the way broadcast journalists cover such incidents and would lead to what some called "The Kiritsis Law" after he was found not guilty by reason of insanity. His acquittal prompted Indiana legislators to amend the law to provide for verdicts of "guilty but mentally ill" and "not responsible by reason of insanity."
Read the full story of the Star here.
Read an account of Kiritsis' attorney here.
content='Anthony G. "Tony" Kiritsis, who made national headlines when he wired a sawed-off shotgun around the neck of an Indianapolis mortgage company executive in 1977 and paraded him through Downtown streets, was found dead in his home Friday.'
name=description>
content="The Indianapolis Star, The Star, News, Sports, Weather, Features, Entertainment, Marion County, Indiana, Indianapolis"
name=keywords>
href="Tony Kiritsis, 72, found dead of natural causes_files/flyout_style.css"
type=text/css rel=stylesheet>
src="Tony Kiritsis, 72, found dead of natural causes_files/style_v3.js">
src="Tony Kiritsis, 72, found dead of natural causes_files/javascript_v3.js">
Tony Kiritsis, 72, found dead of natural causes In '77, he wired a shotgun around the neck of a mortgage company official, paraded him through Downtown, kept him hostage for days. width=1>
January 29, 2005 Anthony G. "Tony" Kiritsis, who made national headlines when Kiritsis, 72, virtually held the city at bay for more than On Friday, he was found dead at his Speedway home in the Efforts to contact family members Friday were unsuccessful. The events of Feb. 8, 1977, elevated Kiritsis to an The incident would forever change the way broadcast Kiritsis confronted Hall in his office at 129 E. Market St., He led Hall through Downtown Indianapolis, surrounded by After negotiating with authorities, he left his apartment The incident proved to be a "watershed" story for Back then, local stations had just acquired the capability Ahern, who had been out to the apartment complex, was back Tom Cochrun, news director at WISH, was a news reporter for "Tony's moods would vacillate from anger, rage and The station's telephone lines were flooded with calls by "We didn't know what to do. Our hands were tied at that But the larger question is whether the station should have In retrospect, Ahern said, the answer is no. "If that thing taught us anything, it's caution and Call Star reporter Rob Schneider at (317) 444-6278. |
src="Tony Kiritsis, 72, found dead of natural causes_files/s_code.js">
language=JavaScript>
Friday, January 28, 2005
Treatment Advocacy Center Newsletter Dec. 24, 2004
TREATMENT ADVOCACY CENTER
Visit our web site www.psychlaws.org
December 24, 2004
******************************
1. SUFFERING MINDS ? Miami Herald, December 12, 2004
2. MENTAL ILLNESS PUSHES FAMILIES TO THE LIMIT - Miami Herald, December 19, 2004
3. WHAT TO DO WITH THE FUNCTIONAL BUT NOT SANE ? Miami Herald, December 19, 2004
******************************
1. MIAMI HERALD, December 12, 2004
[Editor?s Note: In the last two weeks the Miami Herald has turned to those most overcome by severe mental illness and left without treatment by laws that promote psychosis over care and a system that ignores many of the sickest until a law is broken or about to be.
This irrational dichotomy leaves Castleberry Mejias ? about whom a store owner laments, ``But he has no sense'' ? adrift in psychosis. At the end of this piece, you learn on what shore he lands.
This article includes commentary from Rosanna Esposito of our Center.]
SUFFERING MINDS:
The Amount Of Money Spent On Mental Health In Florida Is Among The Lowest In The Country, Leaving The Seriously Ill To Drift Into Oblivion
By Joe Mozingo
He roams his corner of Little Havana, cursing, drinking, pulling his pants down in the street -- a menace with nothing to show for 54 years on Earth but his schizophrenia.
In the small, disordered world of Castleberry Mejias, there is no barrier between real life and the sound and fury of his own imagination.
Mejias has followed the distortions of his mind to jail at least 35 times and an additional two dozen times to Jackson Memorial Hospital's mental health crisis center. He was once arrested trying to light a Dollar Discount store on fire because he wanted a cigar to heat up his ``frozen lung.''
Across Florida, there are at least 25,000 people like Castleberry Mejias -- lives reduced to homelessness and jail by a mental illness that many of them do not understand they have.
Two decades of broken promises and budget cuts have made the untreated poor an accepted staple of life in Florida -- filthy apparitions sleeping in the shadows, muttering aloud, smoking crack to fight off the disembodied voices in their minds.
''The mental healthcare system is in shambles,'' said Michael Mathes, former president of the National Alliance for the Mentally Ill in Florida and current chair of its legislative committee. ``The most needy, the most seriously and persistently mentally ill, fall through the cracks. And people just turn their heads and ignore it.''
Per capita spending on mental health in Florida is lower than in 45 other states, and getting lower. New York spends five times what Florida does. Only New Mexico, Utah, Arkansas and West Virginia rank lower, according to 2001 figures analyzed by the Henry Kaiser Family Foundation.
Treatment Lacking
At a time when psychotropic medications are more effective than ever, an estimated 171,000 people with serious mental illness in Florida do not get the publicly funded treatment they need.
Those with the condition known as anosognosia -- the inability to recognize your illness -- suffer the most, because they often refuse treatment. Only when they commit a crime or pose a threat can they occasionally be forced on medication.
The wretched reality behind the numbers is startling.
Rodney Brown is 51 years old and wears a spaghetti strainer on his head to keep the ''bubble men'' from stealing his thoughts.
He has made a home office out of the oil-stained parking lot behind a Speedy Food drive-through, right next to Interstate 95 near North Miami.
''I put my notes in there,'' he said, pointing to a trash bin. He wears the plastic guard of an old fan as a shield.
Brown has been homeless since he was 18. He has never been treated and is surprised when a visitor asks if he has ever been diagnosed with schizophrenia.
''Like you're crazy or something?'' he said, twirling his finger around his ear. ``Nah.
``When I was walking by the church, an invisible person stuck something in my ear. One of the bubble people. They come in a flying saucer.''
Day and night, burning heat, driving rain, Brown sits in the same spot, flattening cans, smoking cheap cigars, tending a group of kittens. When two of them are hit by cars, he dutifully buries them in the weeds with a spoon.
Sami Ahmed, the owner of Speedy Food and a native of Pakistan, looks after Brown, but can't understand how someone can get so stuck in such a wealthy nation.
''He isn't causing trouble for anyone,'' Ahmed said. 'He needs help. I ask the police, `Why don't you take him to the shelter and get him some treatment?' They say they can't if he doesn't want to go.
``But he has no sense.''
Brown says he would go to his mother's house in Carol City, but the Speedy Food needs him to look after the place.
``I'm going to go see her. I ain't been there for so long.''
He doesn't know the house is vacant. His mother died in June.
Brown is just one of the many psychiatric castaways drifting in the neighborhood.
Three blocks away, Alexander Horn chews a wet cigarette after a heavy storm in July, resting on a sponge of a mattress under a tree off Northwest Seventh Avenue. He has one shoe on, his pants are tied together with electrical wire, and he is typing furiously on a battered husk of an old keyboard.
Horn is 50 years old and has been homeless since his mother died in 1992, the saddest day of his life.
His hands tremble and his tongue circles heavily in his mouth. He is thin as a scarecrow and disoriented, his eyes half-lidded.
''I'm just sitting here reading my Bible,'' he said. `I don't mean no harm.''
The Bible is a crumpled, water-stained Jehovah's Witness magazine. He is reading it upside down.
''I got good sense,'' he said. ''If I want to go to a shelter, I'd go find one.'' When people stop to help him, he thinks they are police trying to put him in jail. He has been there as often as he has been to a shelter, and he likes neither one.
``That's just the way it is, I'm alone. I ain't got no problem being by myself.''
A few minutes later, he is bellowing and slamming at the broken keys of his keyboard, sprawled on a sidewalk as the sane world streams by down on the avenue.
In the eyes of those who try to care for them, people like Horn and Brown are modern-day versions of 19th century lepers, forsaken by society because of a false stigma.
''It's a banishment of people whose symptoms are considered so repugnant and fearful they are judged to deserve their fate,'' said Mathes of the National Alliance for the Mentally Ill.
With more people going untreated, the state's mental health budget is increasingly consumed by crisis.
Under Florida's Baker Act, authorities can involuntarily commit people to a crisis center for 72 hours, at the most, if they are a threat to themselves or others.
Back On The Streets
For most homeless people, this is the only exposure to behavioral healthcare, and it is usually very brief, with no follow-up. The moment the patient is calmed down, he must be released.
Police are appalled to find that the person who was raising hell on their beat in the morning is back on the streets in the afternoon. Families sigh as their tormented son or daughter arrives on their doorstep -- untreated -- hours after being taken away.
''It's a terrible drain on resources, not to mention continued suffering, for people to be cycling in and out of crisis care and never getting treatment,'' said Rosanna Esposito, a staff attorney for the Treatment Advocacy Center, a Virginia-based nonprofit organization.
In 1997, 69,235 Baker Act commitments were initiated in Florida. By 2002, the number had climbed to 105,062.
Tragically, some of those hospitalizations involve the same people going into crisis over and over again. A study by the University of South Florida found that 540 people in the state were hospitalized at least eight times each during a two-year period. And still, no one could force them to take medication.
Psychologists say there is a solution. They point to various ''assertive community treatment'' programs around the nation in which case managers are assigned to the persistently ill and make sure that they find housing and stay in treatment.
But such programs are costly because they require constant follow-ups. And states, including Florida, have provided only limited funding.
''What's really sad is recovery is possible,'' said Xavier Amador, a Columbia University psychology professor and author of a book on anosognosia.
No one witnesses the futility of the revolving door more than street cops.
''You more or less know the addresses already when the call comes in,'' said Miami police Officer Mario Garcia.
One January afternoon, Garcia is on patrol in Little Havana. He is talking about a particularly troublesome case.
''You Baker Act him, you Baker Act him, you Baker Act him,'' he says. ``His name is Castleberry.''
Within hours, a call comes from the Fronton Bar at 12th Avenue and Flagler Street. It is 6:30. Garcia knows the address. He knows who it is.
Castleberry Mejias is already in custody when Garcia gets there.
He threatened to kill the woman who owns the bar with a knife he did not have.
He is charged with felony stalking and taken to the Miami-Dade County Jail.
Paranoid schizophrenia has laid waste to Mejias' life since he arrived from Cuba during the Mariel boatlift of 1980.
He has nothing else left.
He was once a mechanic and father and husband.
Now, he doesn't have a single friend. He has not seen his four children, Claris, Ana Iris, Wilfredo and Gladis -- their names tattooed prominently on his arms -- for 24 years.
`She Never Writes Back'
If he could arrange his thoughts into an unbroken line, he could call 411 and find Claris in New Jersey or his aunt Iluminada in Puerto Rico, for whom he has been searching for more than a decade.
''I wrote to her, but she never writes back,'' he says in jail after his arrest. He shuts his eyes and sobs.
Mejias has heard voices since he was 19. He has been medicated only while in custody, convinced that the doctors give him pills for ''sleeping problems.'' He stops taking them the moment he is free.
''When he takes his medication, he's under control,'' said Miami police Officer Jose DaPena, who has played a cat-and-mouse game with Mejias for years. Without it, ``he's a time bomb.''
Mejias has thrown chunks of concrete at moving cars, lunged at people with broken beer bottles, slammed windows with a metal pipe. A lump on his head commemorates the time a bartender subdued him with a pool cue.
DaPena takes Mejias to the hospital whenever he sees him start to act up.
'I go to the crisis center and they say, `How come you keep bringing back this person?' '' DaPena said. ``I say, `Why do you keep releasing him?'
``The citizens call me. They say he's throwing rocks. What am I supposed to do?''
After his arrest this January, Mejias' stalking charge was dropped, but he stayed in jail on a probation violation as prosecutors looked for a way to get him into treatment. He stayed for nine months. Still, there was no program to accommodate him.
On Oct. 5, Mejias did what so many other Floridians with severe mental illness do.
He went to prison, where he will stay for 4 ½ years.
*****************************
2. MIAMI HERALD, December 19, 2004
[Editor?s Note: In the first piece above the Herald?s Joe Mozingo concentrated on those who are homeless because of a severe mental illness. In the one below, he takes a graphic look at several people stuck in the ?back bedroom.? As is often said, serious psychiatric disorders strike not just individuals but whole families.]
MENTAL ILLNESS PUSHES FAMILIES TO THE LIMIT;
Across The Country, The Families Of The Seriously Mentally Ill Are Stuck In An All-Consuming Struggle To Save The Sick From Themselves.
By Joe Mozingo
Bill Weaver Jr. could see the devil in his old man's eyes. Weaver lashed out at his father's every move and turned his retirement into an endless misery.
Alone together in their condo in western Miami-Dade County, they were locked in a pitched psychological war. One night, Bill, who is schizophrenic, leapt out of the dark and tried to smother 77-year-old William Weaver with a blanket.
Weaver escaped his son and called police, hoping the criminal justice system would help him -- a move he will forever regret.
In the psychiatric ward of the Dade County Jail, Bill dived headfirst from his bunk bed in a manic fit, hit the rim of the toilet and broke his neck. Doctors don't know if he will walk again.
Like so many others, the tragedy lays bare the perils of untreated mental illness and highlights the desperate struggle of relatives to get a disturbed family member into treatment.
Florida's poorly funded and fragmented mental-health system, combined with laws that protect the rights of people to refuse treatment no matter how dysfunctional they are, all but block the path to sanity.
''The law protects the right to be psychotic,'' said Rachel Diaz, who runs a group in Miami called Families of Untreated Mentally Ill Persons. ``Even though, by definition, they are not able to think clearly, we give them that choice.''
At a time when new medications can do more than ever, an estimated 92,000 adults and 79,000 children in Florida with serious mental illness do not get the treatment they need.
The social consequences are disastrous: rampant homelessness, suicide, drug abuse, prostitution, overcrowded jails, tragic police shootings.
But one consequence of a deficient system is kept vigilantly behind the closed doors of thousands of homes: the ceaseless, all-consuming battle families fight to keep those they love from becoming a part of these statistics.
They give up jobs and personal lives. They secretly slip their children medication. They battle to convince the afflicted that they are sick, only to be berated, accused of persecution. They pray when their troubled children disappear for weeks and brace for the storm when they come back.
Protracted Ordeal
Years and decades pass and their adult children are still at home going through the same tortured cycles.
''It's living with a person who insults you, who doesn't obey you, who doesn't appreciate you, who doesn't love you,'' said Diaz, 80, whose husband is schizophrenic. ``It's a miserable life.''
Weaver tries to roll with his son's hostility. Since the accident last year, he visits Bill, now 44, at a nursing home in Allapattah three times a week.
Thursday, he took him a lottery ticket. Bill appreciated the visit at first. But his thoughts quickly took a turn.
''I wish you would die,'' he said, rasping through a dry throat. ``Go home and die. You ruined my life. I really think you are the devil.''
The two argued for a half hour.
''Maybe I'm wasting my time,'' Weaver sighed. ``He doesn't seem happy to see me.''
Not Comprehending
Nationwide, an estimated 4.5 million people suffer schizophrenia and manic depression. Half do not have the ability to understand that they are sick, experts say.
''It's a real dramatic inability to see what's so obvious to everyone else,'' said Xavier Amador, a Columbia University psychology professor and author of the book I Am Not Sick, I Don't Need Help!
``You hear the same stories over and over and over.''
The last year of Maria Santos' life has been a case study in how a family gets stuck in a psychiatric sinkhole.
No matter how many people tell her 28-year-old son Frankie that he is schizophrenic, no matter how many times he ends up in a crisis center, no matter how many times he is locked in jail for disorderly conduct, he refuses to believe he is sick.
''They call me a schizo,'' he whispered to a reporter in November. ``I think I'm just thinking outside the box.''
He lives at his parents' Southwest Miami-Dade home, cannot hold a job and considers himself a ''scholar warrior.'' He thinks God ''inserted'' him on Earth for a divine intervention. He is festooned with grandiose tattoos -- the words ''King One'' cover the side of his neck.
Frankie experienced his first psychotic episode at 18, and he lay naked in a fetal position in his bedroom for days.
Santos is at her wits' end. She watched Frankie's schizophrenic father drive himself into homelessness.
To keep Frankie from the same fate, she is a full-time mom with no end of her work in sight. She has no friends, no hobbies, no job. She's always strategizing, slipping him medication, anticipating the next eruption. The schizophrenia never rests.
And on Dec. 5, 2003, it detonated out of her reach.
A Painful Case
The family was flying back from a wedding in Spain. Frankie began acting up on the plane. Before anyone could restrain him, he punched a passenger in the face several times.
The U.S. attorney indicted Frankie for assault. He was placed under house arrest until his sentencing, scheduled for June 1 of this year.
But for someone with a deteriorating state of mind, rules and court conditions are abstractions easily lost in the throes of psychosis. And that's what happened to Frankie just weeks before his hearing.
''He started going crazy,'' said his stepfather, William Santos. ``He was convinced he was Jesus Christ.''
Frankie stormed through their home, kicking walls, slamming doors, screaming at voices. He took a steak knife to the electronic monitoring device on his ankle.
William called 911.
When police arrived, Frankie shouted obscenities and kicked in the air, as if he were a martial-arts master. Miami-Dade police shot him with an electrical stun gun, handcuffed him and took him to Jackson Memorial Hospital's crisis center.
U.S. marshals removed him the next day. Frankie's acts of psychosis violated the terms of his house arrest.
He spent the next five months in federal custody -- shipped from Miami to Atlanta to North Carolina to Oklahoma -- getting psychological evaluations for an illness everyone knew he had.
His time in custody cost taxpayers at least $10,000, and Frankie came out unmedicated and on the same destructive trajectory he was on before.
At his sentencing hearing on Oct. 15, Maria Santos took the stand and begged the judge to not give Frankie probation. She knew he would violate it.
''He is very, very sick,'' she cried in broken English. ``He is crazy. He need medication for a long, long time. Please, please.''
She wanted the judge to commit him to a state hospital.
She continued: ``For 10 years, he goes to the jail. He goes to my house. He goes to jail. He goes to my house.''
But U.S. District Judge Alan Gold didn't have a legal reason to hospitalize him, and he didn't want to release him altogether. Gold gave Frankie 2 ½ years' probation and ordered him to see a psychiatrist and call his probation officer every day.
He was released that day.
''Back to square one, back to square one,'' William Santos sighed.
At home, Maria Santos immediately began slipping medication into Frankie's Malta Goya drinks. She had no other choice. This kept Frankie marginally in control. But by the end of the month, he spotted some sediment in the glass. He stopped eating and drinking anything his mother gave him.
Earlier this month, Frankie holed up in his room, blasting music. Maria opened his door. Beer was all over the place. He had defecated on the floor.
He was yelling and cursing.
``Get out of my life! Leave me alone! I'm sick of this life!''
''We don't know what to do,'' said William Santos. ``Nobody seems to know what to do.''
Frankie landed -- again -- in Jackson's crisis center, where doctors forcibly injected him with Depakote, a mood stabilizer. His mother took him pizza and clothes, but he glared and blamed her for his confinement.
He was released Wednesday -- back home.
Persistent Stigma
Even as science increasingly reveals that schizophrenia and bipolar disorder are medical conditions, mental illness still carries the false stigma of moral defect, flawed character, weak emotions, murky souls -- Boo Radley locked up in his home in To Kill a Mockingbird, a shame to his family and a boogeyman to everyone else.
''We're a religious society,'' said Irene Darmstedter, of Miami. ``A lot of people think it's evil, that it could be demon possession.''
Darmstedter has to fight to make people understand that her daughter Denise, once an honor student and drill-team leader, didn't choose to drop out of college and sleep on the streets of South Beach.
'My mother is always saying, `Why don't you just give up? She's a bad girl,' '' Darmstedter said.
Denise first showed signs of schizophrenia as a freshman at Florida International University. Her thoughts became bizarre and paranoid. She told her mom one day that the clubs in Miami Beach were drugging young people so the government could control them.
Within weeks, she plunged into psychosis and took off on a bicycle in the night.
No one knew where she was until someone found her, days later, walking along Florida's Turnpike covered in blood. She had cut her wrists.
Denise was taken to the hospital, where she was diagnosed with schizophrenia.
''All she would do is pray Hail Marys and Our Fathers and stare at light,'' Darmstedter said.
Denise was given medication, but she refused to take it. After her release, she drifted into homelessness.
There was nothing Darmstedter could do to stop the decline. She was still grieving over the loss of her son, who died of bacterial meningitis at 15. Now her daughter was dirty and homeless, her nails long and curled ``like a troll.''
''It was a horrible time,'' Darmstedter said. ``We'd see her muttering to herself on Lincoln Road.''
Only when Denise became totally psychotic could Darmstedter get her briefly hospitalized under the state's Baker Act. But each time she calmed down and was no longer a threat, she was released, as the law requires.
Back on the streets, she hurtled toward the next breakdown.
''My son's death was devastating, but this is harder,'' Darmstedter said. ``It goes on and on and on.''
Up And Down And Up
The most painful part for Darmstedter is that she has seen how well her daughter does on the medication. Three years ago, Denise was injected with a long-lasting antipsychotic, Prolixin, and the results were dramatic.
She came back home, applied for a federal Pell grant, went to Miami-Dade Community College and was back to getting A's.
Then a boyfriend convinced her to stop taking medication. ''He told her diet and exercise would take care of it,'' Darmstedter said.
Denise ran away, moved back home, ran away again. She blamed her mother for everything. She broke into her house, vandalized her car, had fits of forced vomiting.
''It was like the scene in The Exorcist,'' Darmstedter said.
Denise bottomed out in November. As Darmstedter and her husband were heading out to a prayer group, she showed up at the door saying she wanted to come home.
Denise, now 29, agreed to take medication. This month, she got a job as a waitress.
Darmstedter is hopeful, but always wary. Lucidity brings its own brand of pain.
''Now she's just so embarrassed and ashamed of everything she did,'' Darmstedter said.
*****************************
3. MIAMI HERALD, December 19, 2004
[Editor?s Note: The preceding stories clearly detail the plight of those homeless with mental illness and the families who give so much to seek treatment for loved ones. The Miami Herald editorial board added its voice, calling for better assessments and increased funding to help those detailed in the previous stories.
We've heard from the Herald?s Board in previous editorials; it weighed in several times for Baker Act reform. Starting on January 1, 2005 those Floridians with severe mental illness who need treatment, have repeated admissions for treatment, and whose illness prevents them from accessing services will be supported by a new law that is designed to offer them more effective treatment. Assisted outpatient treatment will be available in Florida. We are hopeful that this reformed law will bring a happier new year to those it touches, which may very well include one or more of the individuals included in the preceding stories.]
WHAT TO DO WITH THE FUNCTIONAL BUT NOT SANE
Our Opinion: Start With Assessments And Funding For Mentally Ill
Editorial
Throughout Florida -- and especially in South Florida -- thousands of people roam the streets in a perpetual state of psychotic confusion. They rant and rave, hallucinate, react to strange voices and behave inappropriately. To ordinary passersby, they are clearly insane and in serious need of care and treatment by trained professionals.
But to the state of Florida, these homeless wanderers aren't insane enough to be committed to a state psychiatric hospital nor are they violent enough to be sent to a forensic institution. Many of them suffer from a condition called anosognosia -- an inability to recognize one's own illness. To the state, that denial of illness translates to a rational decision by these wandering psychotics to act in their own best interest. Civil libertarians defend the practice as a positive right to be free and independent in our free society.
Psychotic nomads
But something is seriously wrong with this picture. At minimum, these psychotic nomads -- estimated to number more than 25,000 in Florida -- are a nuisance to themselves and to others. They bellow in the streets, bang their heads against walls, frighten children and the elderly, ingest too much alcohol and drugs, and expose themselves in public.
The Herald described the lives of some of these people and Florida's meager spending on care for them in stories last Sunday by reporter Joe Mozingo. One conclusion is inescapable: These victims are a danger to themselves and, potentially, to anyone who comes near them. The disregard shown to them by a wealthy state in a powerful nation that calls itself civilized is a shameful disgrace. That we don't take better care of these marginally functional but clearly disturbed people reflects our own failure to cope with an inconvenient reality.
What is needed is a comprehensive review and reassessment of mental illness in Florida, a kind of statewide audit of needs and services, followed by enough funding to treat all of Florida's mentally ill. Leadership must come from state lawmakers and the governor.
Treatment lacking
Florida's recent history of dealing with the insane is a story of good intentions and bad, with some good results and some colossal failures. Until the 1970s and '80s nearly all of Florida's mentally ill were placed in state mental institutions dedicated to their treatment. Abuse was rampant in many of the facilities, and demands for change led to an overhaul in which treatment of mentally ill people was shifted primarily to private community mental-health centers, the system that exists today. Meanwhile, the state continues to treat violence-prone and severely mentally ill in state-run institutions.
Unfortunately, state funding of the community centers hasn't kept pace with either inflation or the growing number of patients with mental illnesses.
With more precise assessments and appropriate funding, Florida can do a better job of identifying and treating persons with mental illnesses, including those on the margins who think they are sane.
*****************************
Treatment Advocacy Center E-NEWS is a publication of the Treatment Advocacy Center.
This E-NEWS is provided as a public service by the Treatment Advocacy Center. There is no fee. If you would also like to receive a free subscription to the Catalyst, our bimonthly hardcopy newsletter, please forward your mailing address to info@psychlaws.org.
The Center does not accept donations from pharmaceutical companies. Support from individuals who share our mission, however, is essential to our ability to effectively help our most vulnerable citizens. The Treatment Advocacy Center is a 501(c)(3) not-for-profit organization. All contributions are tax-deductible to the extent allowed by law. Donations to the Treatment Advocacy Center should be sent to:
3300 N. Fairfax Drive Suite 220 Arlington, VA 22201 703/294-6001 (main no.) 703/294-6010 (fax)
--------------------------------------------------------------------------------
The Treatment Advocacy Center Newsletter 1/28/05
TREATMENT ADVOCACY CENTER
Visit our web site www.psychlaws.org
January 28, 2005
******************************
1. KENDRA'S LAW-A JOURNEY - NAMI New York State News, December 2004
2. NEW YORK LAWMAKERS CONSIDERING WHETHER TO EXTEND KENDRA'S LAW - National Public Radio, January 25, 2005
3. OUTPATIENT COMMITMENT GARNERS BROAD SUPPORT - Psychiatric News, January 21, 2005
4. TESTIMONY OF JOY SCOBLE - New Jersey Governor's Task Force On Mental Health, January 19, 2005
******************************
1. NAMI NEW YORK STATE NEWS, December 2004
[Editor's Note: Our Center's first major reform campaign was in 1999 for Kendra's Law, New York's pointedly effective law for assisted outpatient treatment. While the effort to secure the measure was just gearing up, a man with untreated schizophrenia pushed Kendra Webdale off a Manhattan subway platform and in front of an oncoming subway train.
The reaction of the Webdale family to her death was as remarkable as it was admirable. Overcoming their indescribable grief and refusing to be obsessed with revenge, they passionately endeavored to prevent the untreated symptoms of treatable illnesses from leading to similar tragedies for other families. The members of the Webdale family became a swarm of fevered advocates for bringing assisted outpatient treatment to their state. At their head was Pat, Kendra's mother, whose continued zeal to help those most overcome by severe psychiatric disorders recently led to her joining the Board of Directors of NAMI-New York. Below are her comments on the law that bears her daughter's name from an article graciously supplied to the E-News by NAMI-NY.]
KENDRA'S LAW-A JOURNEY
by Pat Webdale
Kendra's Law is intended to help keep those who need it on the road to recovery. Just as some people need glasses to maintain control of their vehicles, some need ongoing treatment in order for them to maintain control of their own lives. Kendra's Law, named for my daughter, provides for Assisted Outpatient Treatment (AOT) to help people who otherwise might not survive safely in their community.
I have myself traveled many miles both literally and figuratively since I appeared at a press conference in Buffalo with my husband Ralph and state Attorney General Eliot Spitzer. This November will mark five years since Kendra's Law has been an option for family and friends seeking help for their loved ones. This article is about the journey of Kendra's Law - so far.
The Beginning of the Road
When I heard that Kendra had been killed by a previously violent, noncompliant mentally ill man, I ran around my kitchen asking out loud why Andrew Goldstein wasn't taking his medicine. I vowed to make a difference. My family wrote several letters to Attorney General Eliot Spitzer's office to inquire about the discharge policies of mental health facilities. His response was to tell us about the proposed AOT law he was going to introduce to the state Legislature. He suggested the law be named in honor of Kendra.
Despite the honor, we didn't initially jump at the offer. After all, it wouldn't bring Kendra back to us. Our daughter, Suzanne, a mental health professional, worried that the proposed law wouldn't have any teeth. After much thought, however, we decided such a law would be worth it, if it stopped death and devastation for just one family. Kendra always made herself available to be a friend, to listen to woes, to offer unconditional love. She would expect no less than for us to support a law that could help others.
Going in the Right Direction
After I began advocating for Kendra's Law, my phone began to ring with calls from all around the country. Family members of persons with a serious mental illness began to call and write to me, desperately seeking help for their loved ones. I listened to countless stories, and I learned many things. I learned about others who had died at the hands of a person who had decompensated due to lack of treatment. There was 11-year-old Gregory in New Jersey, 19-year-old Laura in California, 24-year-old Kevin in Michigan. Just recently, a mother in Buffalo was stabbed to death by her son, who was trying to get rid of her "evil eye." She and her husband were Scientologists and were treating him with vitamins.
I heard of the many more who died by their own hands because mental illness had gained control. They included a young relative of mine diagnosed with bipolar disorder who completed suicide three weeks after Kendra's death.
I also learned how persons with mental illness have died at the hands of others - paying the ultimate price for its stigma. I learned of a young man who was having a cigarette behind his group home when he was set upon by a group of youths who dosed him with gasoline and set him on fire. I learned of a young man who died from stomach problems because his doctor thought his symptoms were "all in his head."
Of course, I heard many other stories of "lesser damage." A death is a grievous loss, but so is the loss of a person's future, career path, education, family and love life. I tried to hook people up with resources, and I must have handed out at least a dozen copies of Dr. Amador's book, I'm Not Sick and I Don't Need Help.
I came to the personal conclusion that, for those who need AOT, there were really not two sides to the issue of treatment. For them, it is not a choice between safety and the rights of the individual with mental illness, for mental illness has already gained the upper hand. One must not fall into the trap of advocating for the rights of the illness itself - an illness that can be fatal. We don't advocate for the rights of cancer or heart disease, do we? We must advocate for treatment that will enable individuals to get the control back from the illness. When we enhance the quality of life for even one person, we are enhancing ourselves as a whole. Kendra's Law had the power to change lives - to improve lives - to save lives.
A Bumpy Road
To say the road has not always been smooth would be an understatement. As we expected, there were critics. Those who vehemently opposed Kendra's law were mostly polite in my company, but the implication was clear: I didn't know what I was talking about. Many said the law would do nothing but infringe on the rights of persons with mental illness. What the law infringed on was the right to do nothing, even in the direst circumstances.
After five years, the track record for AOT, when it is properly implemented, has exceeded the expectations of its staunchest supporters. According to the Office of Mental Health's interim report on Kendra's Law, among those who have received AOT services, incidents of hospitalizations, homelessness, harmful behavior and arrests have decreased markedly. Suicide threats and attempts have significantly decreased as have physical harm to self, property damage, substance abuse, and threats of physical and verbal violence to others. Not only that, but the report also found that important changes to local mental health systems have come about as a result of AOT, including enhanced accountability, improved access to services, improved treatment plan development and discharge planning, improved coordination of service planning and improved collaboration between the mental health and court systems. Many of these were unexpected benefits.
One thing is certain: Where AOT has been successful, it is not the program, nor the funding, but the individuals who have embraced AOT and the persons who have done well in treatment that deserve our applause. At the top of my list for special acknowledgement would be the Woodhull Medical and Mental Health Care Center of Brooklyn/Staten Island AOT program. The staff at Woodhull will tell you that it was initially wary of AOT. On day one they had a staff of one and hoped that the phone would not ring. But it did and they progressed from there.
It is the positive attitude of the individuals supporting Kendra's Law, such as Mary Barber, MD, Associate Medical Director of Ulster County Mental Health Department, who make the program successful. These are the people who comply with the law, who take risks despite reservations, who are true professionals and, most of all, who care deeply about their patients.
On the other hand, Kendra's Law does not work if county officials fail to use it, or if they only go through the motions. Going on five years, two counties in New York State have yet to conduct a single AOT investigation, while several counties have only conducted one investigation. In Chautauqua County, a family tried for more many months to get AOT for a man who ultimately set his house on fire and held off the firemen with a shotgun. In Otsego County, a man almost died because his AOT caseworker failed to notify a treatment facility that he was allergic to a medication, even though that fact was written into his court-ordered treatment plan.
It is my understanding that a law is more than just a set of recommendations. Counties and providers must be held accountable in their application of the law, not only in regard to whether they provide services, but in the quality of services they provide. Ensuring a proactive application of the law throughout the state is vital to the lives that are at stake.
The Road Ahead
Where do we go from here?
Improve education: I have heard stories of intensive case managers who don't show up to assist a patient and paperwork that is not completed - small things perhaps to a tired and frustrated worker during a long day, but critical for successful care. These small cracks become a fissure and ultimately a gaping hole. Education should be provided to every person involved with mental health - from the families, police agencies, and ER physicians to mental health providers, case managers. Judges are in a special category of need. I have heard complaints that going to a court for an AOT order is "stigmatizing." Yet the court is there to safeguard the rights of the individual, to decide in an independent manner on a case-by-case basis whether the person qualifies for AOT. The process cannot work, however, if judges do not understand the law, its purpose or how it is supposed to work. Or if they simply don't understand what mental illness is, in the first place.
Advertise: Create an effective advertising campaign. Kendra's Law should be served up on a silver platter to those in need. Tell people what Kendra's Law is and how to access it.
Coordinate services: Those who have successfully navigated the system need to network with those who struggle with it. We need more across-the-board consistencies from the counties. I am amazed at how many resources there are out there, yet dismayed that so many entities continue to work on their own.
National reforms are coming slowly. Many states fight for AOT, but their state NAMIs may or may not support it. We must pull together and make changes that will revolutionize the care of those with mental illnesses and will stand the test of time.
If a family member cannot access Kendra's Law through the mental health system they have the right to file a petition privately. However that is a cumbersome and expensive process. Pro-bono psychiatric and legal services are needed to be made available to such families. Also, the law should be clarified to make this option more viable.
Get support from our legislators: Kendra's Law was enacted with a sunset clause for the law to expire after five years and for a study to be made of its effectiveness. The law expires next June. A new, permanent, Kendra's Law should be proposed early next year [in 2005]. We need to be vocal and gain the support of our legislators for this new law. Those who are in the know because they have a personal situation can be helpful to the cause.
Define the problems and correct them: The Office of Mental Health is conducting the study that was called for by the Kendra's Law legislation. NAMI-NYS also is conducting research. With greater research, I am confident we will find even more ways to increase its effectiveness.
Kendra's sister Suzanne would like to see us prepare a clean-up bill for Kendra's Law. She has proposed a questionnaire to be sent to providers to identify problems. Suzanne points out that different counties have different terms to define similar things such as dangerousness, diversion, enhanced services, and care coordination. They must be on the same page in order to be consistently effective.
The sunset date for Kendra's Law is June 30, 2005, Suzanne's birthday. What a great present it would be to have Kendra's Law renewed and strengthened!
******************************
2. NATIONAL PUBLIC RADIO, January 25, 2005
[Editor's Note: This week Kendra's Law was examined in a segment of Morning Edition, National Public Radio's most popular program. Thirteen million listeners across the nation learned how assisted outpatient treatment can bring needed care to lives turned to havoc by serious mental illnesses. Among those interviewed is Mary Zdanowicz, our Executive Director.
The transcript of the piece is below; the audio stream is available at:
www.npr.org/templates/story/story.php?storyId=4465117 ]
NEW YORK LAWMAKERS CONSIDERING WHETHER TO EXTEND KENDRA'S LAW
MORNING EDITION 11:00 AM EST
Anchor: Renee Montagne
Reporter: Matt Hackworth
RENEE MONTAGNE, host:
In New York, lawmakers are considering whether to extend Kendra's Law. That law requires mentally ill people to receive outpatient treatment. New York state considers Kendra's Law a success, but some patient advocates argue that court-ordered treatment is the equivalent of a jail sentence. Matt Hackworth reports.
MATT HACKWORTH reporting:
Sitting at her wooden kitchen table in her Rochester home, Ann opens a light blue notebook filled with painful reminders of her son's bout with schizo-effective disorder, a mixture of depression and mania.
ANN: This is kind of like a chronological of it, the hospitalizations and all.
HACKWORTH: Ann, who asked her last name not be used, says her son showed signs of illness after graduating high school. He talked frantically and grew more and more removed from the family. Ann says her son was delusional, paranoid, and when she feared violence, she called the police.
ANN: My daughter and I just went into hiding because we were scared to death that he was going to find out that we called the police and that he was going to come after us. That's how significant that bizarre behavior got. We didn't even know who he was anymore.
HACKWORTH: Sometimes police took Ann's son to the hospital. He was hospitalized a dozen times in 10 years, ending up back on the streets with no supervision or follow-up care. Finally, Ann forced her son to stay in treatment using Kendra's Law. Named for a victim pushed in front of a subway train by a mentally ill man, Kendra's Law provides Ann's son with home visits from mental health workers. They make sure he's taking medication and living as best he can. Mary Zdanowicz of the Treatment Advocacy Center says Kendra's Law and other like it are filling a void.
Ms. MARY ZDANOWICZ (Treatment Advocacy Center): This is not just a way to commit a patient to treatment. It also commits the treatment system to the patient. When we closed the state's psychiatric hospital doors and sent so many people into the community, they were really abandoned.
HACKWORTH: Even with Kendra's Law, there are patients in New York state who aren't getting treatment. Some cash-strapped counties set aside little funding for Kendra's Law. It's used more in New York City than upstate and other urban areas still rely on mental health systems and programs that predate Kendra's Law. Many families coping with a mentally ill relative don't know Kendra's Law can help them, and Zdanowicz says patients who may benefit from the outpatient treatment she supports are usually skeptical of treatment anyway.
Ms. ZDANOWICZ: Most of the people in these programs are people with schizophrenia and some with bipolar disorder, and the thing that's common to those two illnesses is that there is a certain portion of those people who just don't realize that they're ill, and so because they don't think they're ill, they don't want to be treated.
HACKWORTH: In about a third of Kendra's Law cases, patients who refuse treatment at home are forced by the court into a hospital for observation. Advocates say without treatment, those who refuse help are at greater risk for violent altercations and homelessness. But some challengers to Kendra's Law see refusing treatment as a patient's individual right. George Ebert works for the Mental Patients Liberation Alliance, one of about 100 grassroots groups fighting outpatient treatment laws across the country. Ebert says even with a mandatory court hearing where patients and their attorneys can fight placement in such programs, outpatient treatment laws still violate civil rights.
Mr. GEORGE EBERT (Mental Patients Liberation Alliance): Would we be considering people that haven't broken a law, haven't been charged with a crime, yet are being made to do something that someone else doesn't have to do, it's civil liberties?
HACKWORTH: Kendra's Law has already survived a court challenge that argued it violates civil rights. The New York law is up for renewal in the spring and Ebert says his group will protest keeping it in place. A state study found largely positive results for Kendra's Law which is one reason lawmakers are expected to extend it. Family members like Ann whose son receives treatment under Kendra's Law say they're hoping it's extended. Ann says her son has been out of the hospital for more than a year and visits from mental health workers are the only way he'll take his medication.
For NPR News, I'm Matt Hackworth.
MONTAGNE: This is NPR News.
******************************
3. PSYCHIATRIC NEWS (Vol. 40 No. 2), January 21, 2005
[Editor's Note: Among the progeny of Kendra's Law is Kevin's Law, an analogous Michigan measure that was also forged by a tragedy. Kevin's Law was passed, became law, and took effect all in the waning weeks of 2004. Psychiatric News, an official publication of the American Psychiatric Association, reports on the new law and uses it as a springboard for a wider examination of assisted outpatient treatment.
Note: Forty-two states, not 24 as in this article, have some form of assisted outpatient treatment.]
OUTPATIENT COMMITMENT GARNERS BROAD SUPPORT
By David Milne
Michigan joins the ranks of states mandating outpatient psychiatric treatment as an alternative to incarceration and homelessness for some mentally ill individuals.
Michigan has joined 24 other states in giving courts, police officers, psychiatrists, mental health professionals, and families with a means of forcing people with mental illness into treatment rather than jail.
Wayne Creelman, M.D: "The outpatient commitment law...is especially helpful in the care of patients when substance abuse is a complication to underlying psychiatric pathology."
The law, signed by Gov. Jennifer Granholm (D) late last month, goes into effect immediately.
Named for a college student in Kalamazoo killed by a person who had been in and out of mental health care, Kevin's Law allows judges to order treatment for people who are not following a regimen recommended by a psychiatrist or mental health professional.
People may be subject to such court orders only if they have been hospitalized or imprisoned in the previous three years or acted violently toward themselves or others in the previous four years.
Since the nationwide closing of psychiatric hospitals beginning in the 1970s, states have had little power to mandate mental health care, unless someone is dangerous or convicted of a crime. Family members and advocates for mentally ill individuals in Michigan have pushed for Kevin's Law since 2001. Public awareness that the state's mental health care system is broken helped create a consensus for the bill this year.
State Sen. Tom George (R), who introduced the bill, said that it will improve public safety, especially in urban areas, where patient treatment is concentrated, and provide the treatment that people with mental illness often have trouble getting.
A similar law in New York State, Kendra's Law, resulted in a 83 percent reduction in arrests, an 86 percent reduction in homelessness, and a 67 percent reduction in poor medication compliance among people ordered to receive treatment, according to the New York State Office of Mental Health. George is the only physician in the Michigan Senate and has a brother who suffers from mental illness.
The constitutionality of similar laws in other states has been challenged, so far without success.
"I think a good job was done by advocates in working with the sponsors on rights protection issues under these new bills," Mark Reinstein, Ph.D., president and CEO of the Mental Health Association in Michigan, told Psychiatric News.
"The potential downside is that this area can't be perfectly legislated. We could spend the rest of our lives always coming up with one more `what if' that hadn't previously been covered. So the question becomes: How well will our first crack at this work?"
While many in the mental health community believe the legislation is needed, they also recognize that some fine-tuning may be in order in the next couple of years.
Reinstein claimed that Michigan simply has way too many problems with incarceration and homelessness of untreated mentally ill populations to sit back and not take this step.
"I realize that some persons with mental illness are against mandated treatment," the director of Michigan's Alliance for the Mentally Ill, Hugh Huebl, M.D., told Psychiatric News. "But when you consider that Kevin's Law pertains to persons who already have become a part of the criminal justice system because of their illness, it is hard for me to see any downside to mandated treatment under those circumstances."
Huebl thinks more attention should be directed to families struggling to cope with members who are psychotic, delusional, and sometimes paranoid and whose behavior is grossly detrimental, inappropriate, abusive, and socially unacceptable. He said these individuals often do not realize they are ill.
"I have recently dealt with several such cases, and if they do get a court order and their loved one is picked up by the police, most of time it is fruitless because the criteria of imminent danger to self or others is too stringent, and either the person is not admitted to a facility, or they are kept for too short a period of time, or the judge turns the person loose and they are back where they started from," he explained.
Huebl said that mothers are often left holding the bag, because of estrangement of siblings, husbands, or ex-husbands. Some community mental health agencies are opposed to providing more appropriate care, because it will cost more money, which only complicates the problem.
"I think the present way of dealing with these situations is unconscionable and inexcusable. I am all for rescuing and mandating care in these circumstances. If it were me, and the person refused medications, I would confine them indefinitely until they finally would come to realize that they needed help."
In one judge's opinion, Kevin's Law needs to be fine-tuned to make it more practicable. "Some requirements, such as the need for two additional witnesses, could make it difficult to implement," Milton Mack, chief judge of the Wayne County Probate Court, told Psychiatric News.
The law requires a lay witness to testify to the facts of the case and an expert witness to determine whether the person is mentally ill and, if so, whether the person meets the criteria for involuntary inpatient treatment. In addition, testimony is needed from an expert witness aware of certain prior acts by the person. The treating physician would know that but never appears in court, according to Mack.
"Getting an expert witness to testify about the person's history sounds simple, but you need to get someone on the stand who has intimate knowledge of the person to do that," he said.
He believes the law would work better in some rural counties where witnesses can be easier to find. But in high-population counties it might run into difficulties.
"Sometimes I think I need to be Dr. Mack as well as Judge Mack because the statute appears to give me the authority to decide what kinds of medications should be administered. And at the hearing I can enter a judgment regarding case management."
Under the law a judge can decide whether blood and urine tests should be used to check compliance with the effectiveness of medications, whether the person gets individual or group therapy and attends a day or partial day program, whether the person gets educational or vocational training, and whether there should be supervised or unsupervised living arrangements.
"A doctor doesn't have to make these decisions. I do. And I'm not a doctor."
Mack agreed with the Mental Health Commission's recommendation that if someone has a mental illness, the judge should get an order for treatment for 180 days. If the person gets better in the interim, he or she can have another court appointment and have the order rescinded. After that the community mental health agency would manage the patient.
"Being able to order outpatient treatment under Kevin's Law is a good idea because we live in an outpatient world. But unfortunately the Mental Health Code is an inpatient model," said Mack
Mack doesn't feel comfortable being so closely involved with what medications a person with mental illness should have.
"It's not my role or expertise. I don't think the patient will be well served by me making that decision."
The president of the Michigan Psychiatric Society, Wayne Creelman, M.D., told Psychiatric News that the district branch "has been very supportive of Kevin's Law all along."
"As always with legislation, the devil is in the details of its implementation," Creelman said. "The outpatient commitment law, however, is especially helpful in the care of patients when substance abuse is a complication to underlying psychiatric pathology in that [the law] allows caregivers to assist their patient population in the least-restrictive environment possible."
******************************
4. TESTIMONY OF JOY SCOBLE, January 19, 2005
[Editor's Note: After looking at one law that has been facilitating treatment for five years and another that has just begun doing so, we now turn to the effort to bring assisted outpatient treatment to New Jersey. Last week we shared the brave testimony of Cathy and Mark Katsnelson before the New Jersey Governor's Task Force on Mental Health. Below is that of Joy Scoble. Her brother's plight is also dire and indicative of laws that irrationally withhold treatment from those whose will has succumbed to psychiatric illnesses.]
BEFORE THE NEW JERSEY GOVERNOR'S TASK FORCE ON MENTAL HEALTH
Mr. Chairman and Members of the Task Force,
My brother has recently been released from Northern State Prison. He completed his 4 year sentence and was maxed out. Since his release, he's moved from location to location because he has had fits of rage and the family member or friend, who has been so gracious as to support him, no longer feels comfortable having him live with them. Today, my brother is living on the streets. Today, in these freezing temperatures, my brother does not have a place to call home. My mother cries constantly on sleepless nights because she is unable to allow my brother to visit her at home.
About 4 or 5 years ago, my brother attempted to attack my father in the middle of the night with a broomstick. During this battle, my brother claimed that he was going to kill my father and when that was done, he was going to go back into the house and kill everyone else. This, coming from a brother with whom my sister and I have been so close to in our childhood years, was shocking to hear. The reason why I do not hold this against my brother is because I know it was something that was triggered by his mental illness. When he has a fit of rage, as he does randomly, there is no catalyst that sets it off.
For about 5 or 6 years now, my family has desperately attempted to get him help for his mental illness. My mom has pleaded to a judge at one point, to try and have him committed. This was unsuccessful because he's an "adult" who cannot be forced into help. For years, he's been thrown out of Salvation Army and YMCA housing because he's been in fights with other residents. During his 4 years at Northern State Prison, he's been in multiple fights and has been placed into solitary confinement more times that I can count. At one point, his doctor had put him on Risperdal and when family had visited him, there was a significant change in his attitude. He had seemed completely "normal." Only a few visits after that, he converted back to his depressive state. After questioning him about the medication, he explained that he didn't think it was working, so he decided to stop taking it. After that visit, he had gotten into another fight.
While my brother was finishing up his sentence, I had received a letter in the mail. It was from a gentleman who had shared a jail cell with him in the past. This man had been released from jail and he wrote to me because he was concerned for my brother. He noticed that my brother had reverted back to his depressive and destructive state and was wondering if he had stopped taking the medication.
Today, everyone who's met him is convinced that he needs extreme help for his mental illness. When he gets into a fit of rage, he does not make sense and he appears to be dangerous. I've recently contacted my local city police station to inform them that my brother is living on the streets and that if he were to get into any trouble, I would prefer it if he was taken to a local hospital for evaluation on his mental illness. When I spoke to the Lieutenant, he informed me that he remembered my brother from previous incidents. When I explained that he's having fits of rage, this officer assured me that if they found him, they'd take him into a hospital. The next day, my mother called the police on my brother because he was trying to get into her house. The police officers showed up, and said they couldn't take him anywhere against his will.
This is why I've felt so helpless. Numerous times, I've contacted hundreds of people in law enforcement and mental health offices, but have been unsuccessful in receiving advice. As I've been told, I cannot get help for my brother until he attempts suicide. Which, in my opinion, is sad. It's sad that society will not help others until extreme measures are taken.
I wholeheartedly support assisted outpatient treatment and hope that New Jersey will take the step that so many other states have taken in improving mental health issues before anything extreme happens. Before lives are taken from innocent people who are either victims or are those who cannot ask for help themselves. I implore you to consider giving individuals another chance at life.
******************************
Treatment Advocacy Center E-NEWS is a publication of the Treatment Advocacy Center.
This E-NEWS is provided as a public service by the Treatment Advocacy Center. There is no fee. If you would also like to receive a free subscription to the Catalyst, our bimonthly hardcopy newsletter, please forward your mailing address to info@psychlaws.org.
The Center does not accept donations from pharmaceutical companies. Support from individuals who share our mission, however, is essential to our ability to effectively help our most vulnerable citizens. The Treatment Advocacy Center is a 501(c)(3) not-for-profit organization. All contributions are tax-deductible to the extent allowed by law. Donations to the Treatment Advocacy Center should be sent to:
3300 N. Fairfax Drive
Suite 220
Arlington, VA 22201
703/294-6001 (main no.)
703/294-6010 (fax)
Wednesday, January 26, 2005
Story Titles, Leads, Themes, Plots, Ideas
The Mentally Ill Offender
Dollars and Sense
Locations
Treatment in Jail
Politics Link 1
Commissary Fund Link 1
ICAN
Egos
NUVO
Suicide Tank
Federal Court
Love Ones of the Rich and Famous
Commitments Link 1
Mysterious Deaths
Channel 13 News
Dept. of Corrections
Habitual Criminal Act
Mayor's Task Force on Dangerous Mentally Ill
HAND
Conferences
Case Study One
Case Study Two
Jake's Law
a WIP [a work in progress]
Zero Tolerance Rules
Red Zones
Enhanced Prosecution Zones
The Prosecutor's Top Ten Offenders' List
Cast of Characters
Indiana Consortium For Mental Health Services Research Link 1
Judy Spray, Public Defenders' Agency Link 1
Mike Trent, Midtown MHC
{kind=link}
Lee Stephan, Gallahue MHC
Jim Frank, Attorney Star Photo
{kind=link}
Photo
{kind=link}
Eric Wright, PhD Associate Professor IU
{kind=link}
Daneille Gaughan, Public Defenders' Agency
Judge Evan Goodman Photo
{kind=link}
Judge Barb Collins Photo
{kind=link}
Judge Steven Eichholtz Small Photo Photo Link 1 Link 2 Link 3
{kind=link}
{kind=link}
Luanne Pyle, BehaviorCorp.
Dr. Carol Gardner, Professor,IU
{kind=link}
Dr. Lee Luskin, Professor,IU Link 1
{kind=link}
Former Sheriff Jack Cottey
History of Jack Cottey
{kind=link}
Photo
{kind=link}
Link 1 Link 2 Link 3 Link 4 Link 5 Link 6 Link 7
{kind=link}
Link 8 Link 9 Link 10
Fran Quigley, Director, ICLU
Ken Falk, Attorney, ICLU
Former Prosecutor Scott Newman Link 1 Link 2
Former Mayor Stephen Goldsmith
Mike Grubbs, Attorney Photo
{kind=link}
Lincoln Plowman, Jail Medical Director Photo
{kind=link}
Marianne Halbert, Public Defenders' Agency Link 1
Judge Taylor Baker Photo
{kind=link}
Jail Medical Officer
Jail II Commander
Community Corrections
Lynn Carson, Mental Health Association
MH Commissioner
Judge Sheila Carlisle Photo
{kind=link}
Lilly
Alan D. Schmetzer, MD
Photo Link 1
{kind=link}
Eugene S. Turrell, MD Indications of Change in the Dangerous
{kind=link}
Dr. Tom Hoshour Photo Link 1 Link 2
{kind=link}
A Tale of Two Lawyers- Newman and Quigley
Commissioner Vickie Yaser
Vicky Ransberger
Poor Public Defenders' Agency
Judge Carr Darden
Alan Schmetzer, MD
Contact Info
{kind=link}
Romeril
Tuttle
Introduction
[Psychiatric Assertive Identification and Referral Program]
It has now been about ten years since the PAIR Program was started. Some things get hazy with the passage of time, but others become more clear. One of my ideas is to write as much about this local sociological movement to prevent further clouding of the history. I believe it is important and more than an ego boost for any individual. The most prominent issue becoming clearer each day is that persons who actually had little to do with the work of establishing the PAIR Program are purposely, or inadvertently, taking credit for it. [see example 1] There should be a clear accounting of the process as much as possible so others can learn from it. If the emphasis is on promoting one’s self the cause is lost.
And the cause is just and worthy of further work, study, and consideration.
I understand this may be a monumental task and that I am not infallible with my memory. I want to consider it an ongoing work and to get the input from others as much as possible. I plan to keep this journal on my computer as well as my website and to start a blog.
I hope to write this account as accurately as possible with as many names and sources as I can remember. It is my hope that such an account can aid any in doing research of the facts and to establish a body of knowledge that we all can learn from.
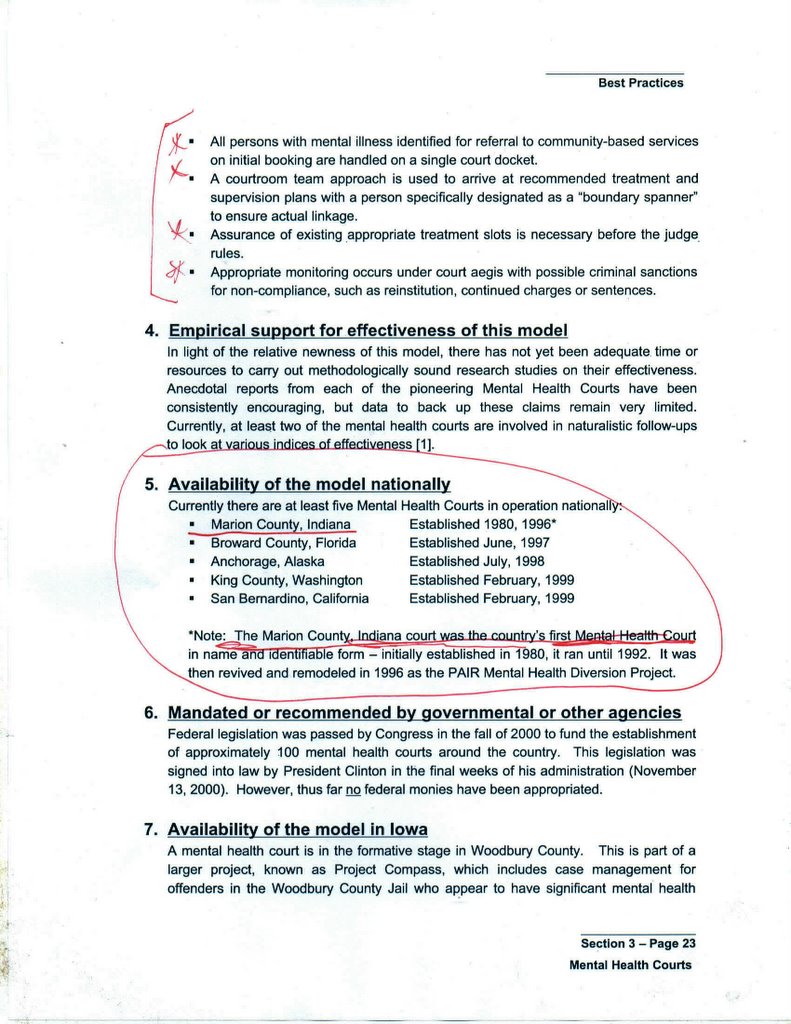
"In 1996 Marion County, Indiana, started the Psychiatric Assertive Identification Referral/Response (PAIR) Program in Indianapolis, which many consider to be the nation’s first mental health court. This initiative is a comprehensive pre-trial, post-booking diversion system for mentally ill offenders. In 1997 Broward County (Ft. Lauderdale), Florida launched the first court to be formally called a specialized mental health court." Quoted from here.
The quote above is somewhat in error. It is from a national publication and has been cited many times. While there had been one form or another of informal mental health diversion since the early 1980's, PAIR was not formalized into a concise program with rules and vested stakeholders until 1996. The PAIR Program shares much of its history with the Mental Health Court of Judge Evan Goodman. So in some aspects, the program is much older. [see reference] [See Report from Iowa naming PAIR as a "best practice model"]
{kind=link}
Of special note, the literature frequently is wrong about the first mental health court being in Florida in the 1990's. The first mental health court was at Wishard Hospital in Indianapolis in the early 1980's. The presiding Judge was Evan Goodman. The court was set up in the small gym and basketball court we use to use as an exercise area for the inpatients. There are even national stories about this legal court being held on a basketball court. There is even a photo of Judge Goodman with a basketball net. All of this was from the 80's, way before all of the current interest and growth in mental health courts. I was fortunate to be present during that time and joined the forensic mental health team in the mid 80's.
The psychiatrist during the early years of the court was Eugene S. Turrell, MD [deceased] [Read Turrell's Treatment Goals]. I believe there is some published work of his about this historic time.
I came up with the name PAIR [Psychiatric Assertive Identification and Referral] Project in 1995.
The mental health court was at Wishard Hospital from the early 80's until the early 90's. I joined the specialized mental health team which worked with the court in the mid 80's. This team was called the Forensic Team. Its duties were to over see the patients who were on out patient commitment and refused to follow the court's order. Another duty of the team was to work with the criminal courts, the jail, the prisons, the parole department, and the probation departments.
In a consent decree with the jail, ICLU, and the US District Court, I was designated to work with the suicidal inmates once per week at the jail in a group session. The work was with the SP inmates from 1987 to 2000.
I went on a six month leave in 1989 to work with the State of Indiana as a consultant with the CHOICE Program. I acted as a consultant for the placement of the mentally ill in the community rather than placing them in an institution.
While I was on leave, Evan Goodman, the Presiding Judge, of the mental health court, was promoted to the position of head judge over all the administration of the then municipal courts [ about 18 courts in all].
Since many of the staff were promoted and transferred, I was asked to fill the position of Court Liaison for Midtown MHC and the Marion Co. Courts. I continued my work of overseeing the 600+ commitments to Midtown MHC, as well as running the group sessions at the jail for the suicidal inmates.
It was during this period that I developed another important contact. In 1987, I began work with the Midtown MHC's ADAPT program. It was a program on anger management in cooperation with the courts, social agencies, and the Marion Co. Prosecutor's Office. This would lead to me being vice president of the Indianapolis Domestic Violence Network and on a policy committee for Prosecutor Steve Goldsmith in developing policies to handle domestic violence. I believe I contributed a lot to this committee as the problems of mental illness and domestic violence often overlap. {Listen to a radio inteview where I describe this program.]
Later when Goldsmith became mayor, I was to serve on his committee looking into the problem of the dangerous mentally ill in the community and how to develop an effective plan.
We went through several judges at the mental health court. Judge Taylor Baker [See Link 1] was there for a while, but the job did not suit his temperament. Judge Carr Darden stayed for about one year until his promotion. Judge Darden is now on the Court of Appeals.
{kind=link}
Judge Steve Eichholtz came last and remained about one year. He often had Commissioner Vicki Yaser also preside over cases. Later, he supervised the closing of the specialized court and the transfer of its unique functions back to the Probate Court.
It is during this time of transition back downtown, I had the opportunity to work with a lot of the courts, the public defenders' agency, the lock up, and the prosecutors' office. I made many acquaintances and friends. I found many advocates for the mentally ill and allies in working to make the system better.
I was contacted by the Johnson County Prosecutor's office and was recruited to do a private domestic violence program for them. I would work as a consultant for about three years with Johnson County.
It was about this time that I was deemed an expert witness and recruited by the Public Defenders' Agency to do private consulting with them and write alternative sentencing reports and recommendations.
Of special note, Judge Eichholtz helped supervise the investigation of several deaths at Central State Hospital, as the deceased patients were on civil commitments out of his court. [On a side note--I personally knew many of these patients having worked at Central State Hospital from 1975 to 1978. Some I even knew from my childhood as my mother was a nurse there.]
It was during this turbulent time that mental health attorney and advocate Jim Frank challenged the state's right to keep the mentally ill hospitalized without giving them the best available medication. At the time, clozapine was seen as a miracle drug for many of the chronically mentally ill with negative symptoms. This were the patients who were frequently in Central State Hospital. Attorney Frank argue if the state was gong to force these people into treatment and to keep them locked up, the state should give them the best available treatment. The problem was that this medication cost anywhere from $10,000 to $20,000 per year, per patient, and one of the possible side effects was death, if not carefully monitored.
Judge Eichholtz heard the case to compel the state to provide clozapine. Doctors gave testimony that there were dozens of patients who would benefit from this treatment. The judge issued an order for state to provide this treatment even though it said it could not afford it.
Some have argued that this was the true reason for the shut down of Central State Hospital: that the state had closed the hospital in an effort to try to pass the ever increasing expense of caring for the mentally ill onto the federal government. Many advocates had claimed that medications and services that were not covered by the federal government while a person was in a state hospital, would be covered if the were "treated" in the community.
It was around this time that Gov. Evan Bayh made his visit to Central State Hospital to make a personal survey. He did not like what he saw. He ordered the hospital to be closed within one year.
A big contributing factor to the start of the PAIR Program was the influence of politicians to keep their private slush funds and make it seem like the monies were being used for the public good. [read A Tale of Money]
Three other big influencing factors would come into the formation of the PAIR Program. One was some Indiana Supreme Court rulings and the other was the formation of a research group to study the closure of Central State Hospital. The final influencing factor was the election of Scott Newman as County Prosecutor.
A few years earlier the Indiana Supreme Court had ruled that Marion County's method of identifying the mentally ill by placing a charge on them as DOC? [disorderly conduct because of mental illness] was unconstitutional. This simply meant that a person accused of a crime faced charges or not, but it often lead to the mentally ill patient being held in the jail for sometimes up to a year and often without treatment.
The other Indiana Supreme Court ruling which affected the history of PAIR was the TT ruling. It basically said that the mental health court had no authority to enforce its orders. The mental health court judge had up to that time, the power to find persons who did not follow his orders, in contempt. He could then order sanctions ranging from incarceration, more intense monitoring, home arrest, etc. After the Supreme Court ruling, the mental health court judge had no power to enforce its orders and no ability to enforce the rules of an out patient commitment. As a result, perhaps hundreds of patients quit treatment without any supervision. For example, Midtown MHC had over six hundred out patient commitments. On any given day, 50% were non-compliant with the court's order to some degree. The only recourse after this court ruling was to hospitalize noncompliant patients. Midtown only has a couple dozen of inpatient beds. The other problem is that patients who stop their treatment may not have their symptoms manifest for months. By the time many of patient's symptoms had worsened, their commitment would have been dropped.
The other big court ruling was the decision that psychiatric medications could only be forced in the treatment of an illness and not for abnormal behavior. A much quoted opinion about the side effects of tardive dykinsia was published. This ruling and opinion had a chilling effect on the psychiatric community. There is no blood test for mental illness. Diagnosis is often made on the basis of behavior. Persons who exhibited psychotic behavior were frequently arrested. It was easier for many mental health providers to wash their hands of the problem and let patients go to jail. It also become fairly common for inpatient facilities to call the police when a psychiatric patient acted up on the ward. These patients would be arrested and transferred to the jail, often in a psychotic state.
Another major influencing factor was the formation of the research program from IU. This did several things to enhance the development of PAIR. Just the fact that they were studying the program and the problem lent some legitimacy. Other factors included the prestige of many of the professional people to be part of the literature and perhaps be named as co-authors. This is important in both the legal and psychiatric field. The final factor was that because of this research, the program might qualify for federal funding. This proved irresistible for many of the stakeholders---the ability to be paid for what they were already doing.
The final major influencing factor which brought about an alignment of forces to permit the development of the PAIR Program was the election of Scott Newman as prosecutor. The National Law Journal called him the "kamikaze prosecutor". I had met him when he first went to work as a young deputy prosecutor when he did some time in the mental health court. He was arrogant, brash, rude, and totally unsympathetic to the problems of the mentally ill. I will always remember him as the worst prosecutor we ever had in the mental health court. [Read more about him in the essay "A Tale of Two Attorneys"] Many professional people could not understand how such a person could be elected, and even Newman himself has been quoted as saying, "even a trained monkey could have won the election that year."
Newman used this slush fund to his advantage while seemingly persecuting the poor and mentally ill because the public defenders' agency was underfunded and understaffed [ see PDA Link]
Newman did four things which were devastating for the plight of mentally ill and the enlargement of the problem of criminalizing the sick. They are:
1. The establishment of "no tolerance zones" or "red zones".
2. The establishment of the no tolerance for plea bargaining and the goal of seeking the maximum sentences even on misdemeanor offenses.
3. The publishing of the "top ten list" of misdemeanor offenders who he publicly stated he wanted to get and put in prison forever. The problem with this list was that at least eight of the top ten were persons with severe mental illness or mentally retarded.
4. The establishment of a policy to rid the downtown of homeless persons, with increase prosecution for trespassing, disorderly conduct, or pan handling.
The Newman factor was the most disturbing to me personally, but has not gotten a lot of press. How could one man persecute and hurt the mentally ill unfettered? I will explore this issue in other essays. [read related article on Scott Newman]
The next stop for many of these patients was the county jail and on to prison. With the passing of "The Kiritsis Law" , the general public showed that it was not symathetic to the mentally ill. The Kiritsis Law was the establishment of the doctrine that a person could be "guilty, but mentally ill." Most of the public, and even today, believe that when a person is found "guilty, but mentally ill", they are kept in a special humane place within the prison system and given treatment while they are contained from society. This is not true and many, if not all, of these individuals are treated worse and more cruelly than if they were just found guilty and given the maximum sentence. Some of these mentally ill inmates would in effect be tortured during their years of incarceration and then be released unsupervised back into the community and often untreated. Many in fact came out without even the supervision of parole as they had often acted up the whole time of their incarceration and thus had served the maximum sentence. There is no provision in Indiana law to add more sentences and parole because of mental illness. What is especially sad here is that frequently, the Department of Corrections, would go to a local mental health hospital and explain that a mentally ill inmate was about to be released. The DOC would ask the center to commit these individuals for treatment. The same individual who had often been mistreated and neglected for years.
Now this is the true setting for the formation of the PAIR Mental Health Program. The state hospital is closing. There is a back log of patients in the community who need hospitalization. Many psychiatric patients are being arrested for acting out with the encouragement of the "kamikaze prosecutor". The mentally ill who have been in prison for years are being released, untreated and abused, back to the community without supervision. The mental health specialty court is shutting down.
****I will continue later*****3/4/05*********
The PAIR Program is cited in the virtual "who's who" of mental health diversion programs listed here.
![]()